Common Bile Duct Stones - Ultrasound
by Julien Puylaert¹ and Robin Smithuis²
¹ Medical center Haaglanden in the Hague and Academical Medical Center in Amsterdam and the Alrijne hospital in Leiden, the Netherlands
Publicationdate
This article is a brief overview of the video presentation on common bile duct stones by Julien Puylaert.
You can watch the full presentation by clicking the accompanying YouTube link for detailed explanations and additional patient examples.
For critical comments and additional remarks: [email protected]
Introduction
Click on the image to go to the full presentation by Dr Julien Puylaert.
Or continue reading and watch the presentation later.
Anatomy

At the liver hilum the common bile duct (CBD in green) lies anterolateral of the portal vein and the hepatic artery, while the hepatic artery proper runs anterior and slightly to the left of the portal vein.
As the right hepatic artery branches toward the right lobe of the liver, it typically runs posterior to the CBD.
In its distal course, the CBD runs parallel to the superior mesenteric vein. This can be helpful in identifying the CBD.
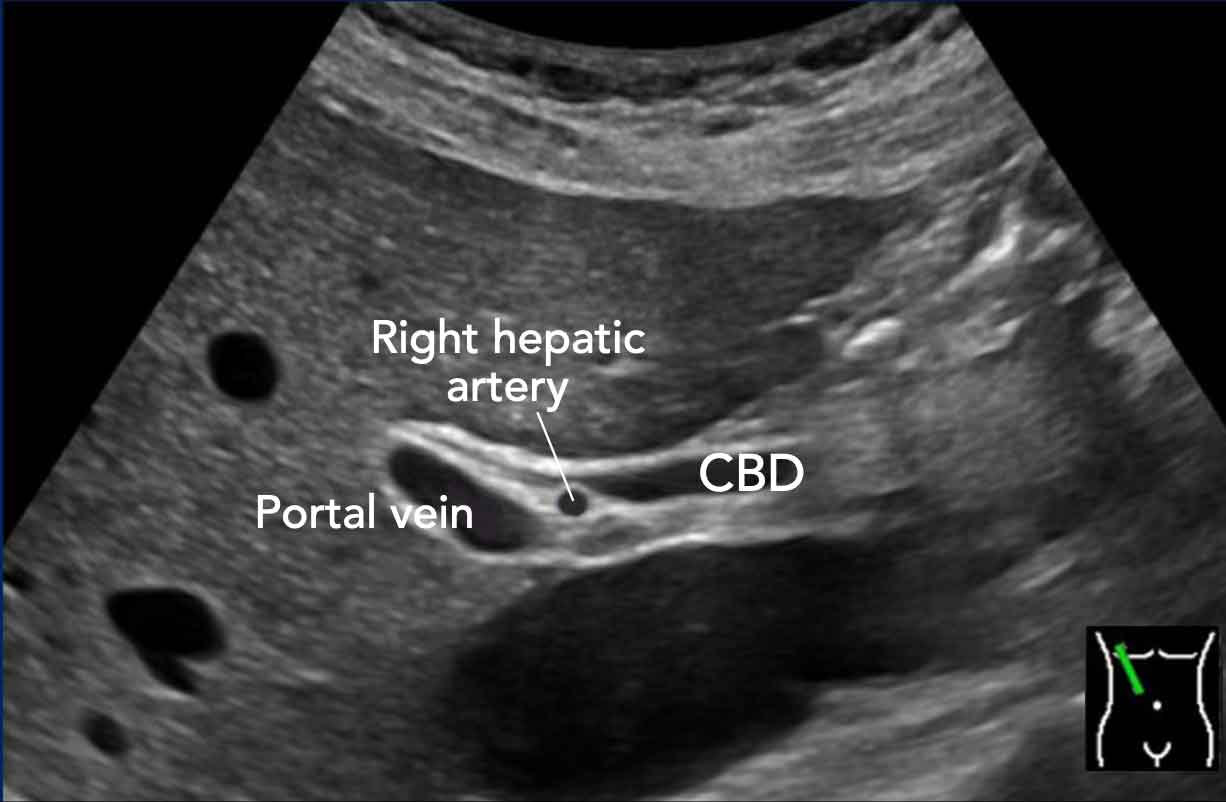
In this longitudinal view, the right hepatic artery is visualized interposed between the portal vein posteriorly and the common bile duct anteriorly.
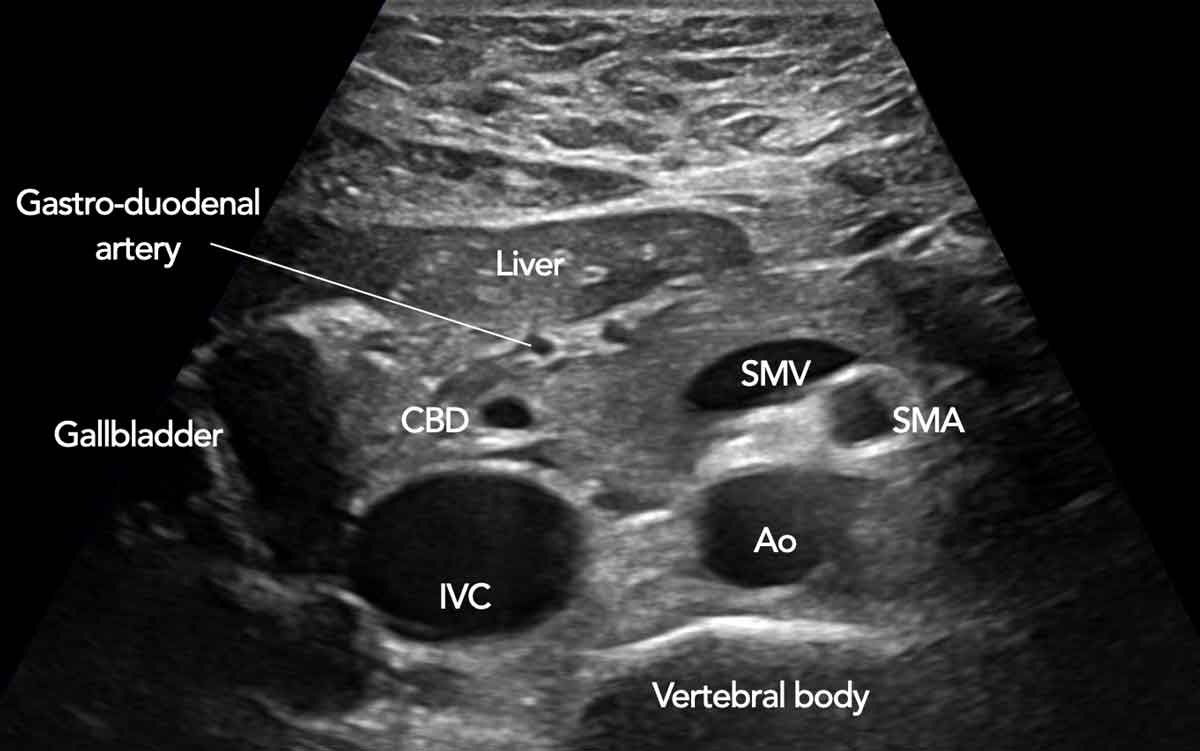
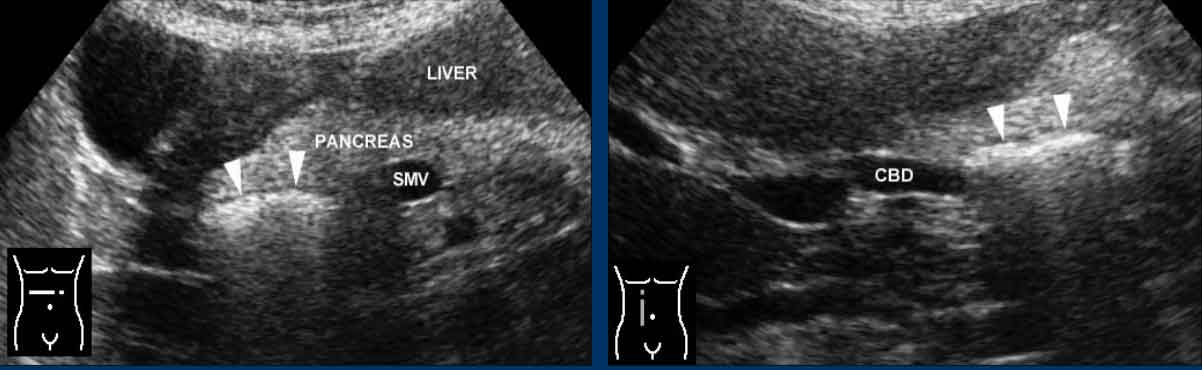
US anatomy in axial plane
Note the position of the distal CBD in the pancreatic head, and the position of the superior mesenteric vein (smv).
The gastroduodenal artery is seen more anteriorly in the pancreatic head.

SMV trick
When you identify the SMV in the axial plane, rotate the probe 90 degrees to visualize the SMV in the longitudinal plane.
Then angulate the probe to the right to find the CBD (scroll image).
 Click on image for enlarged view
Click on image for enlarged view
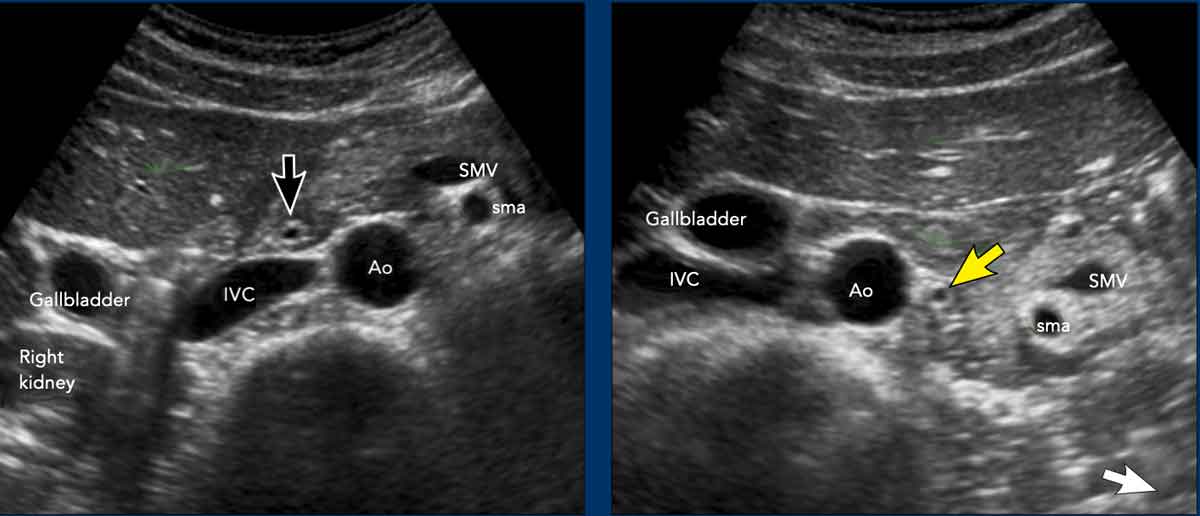
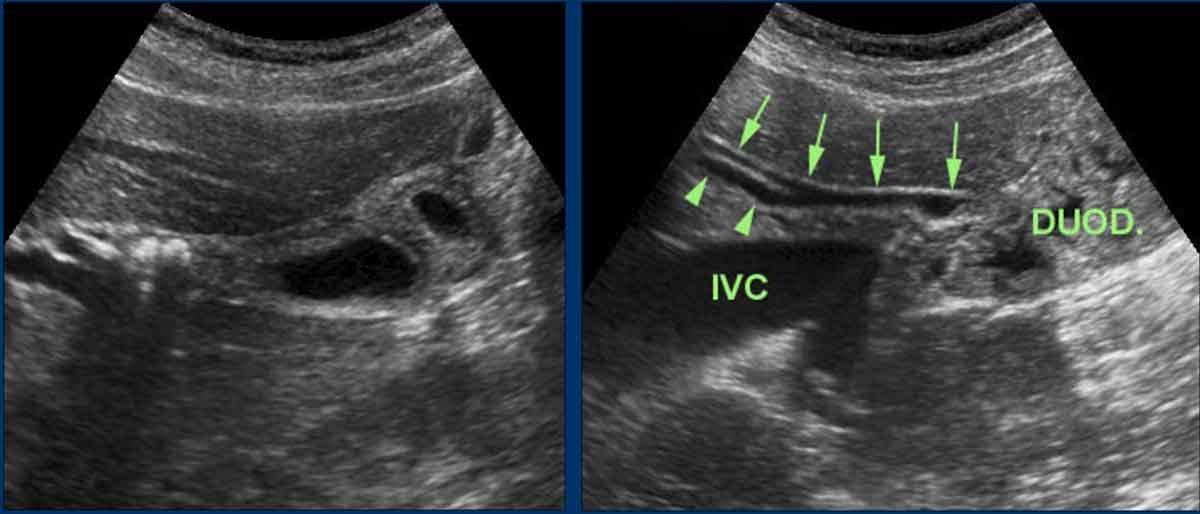
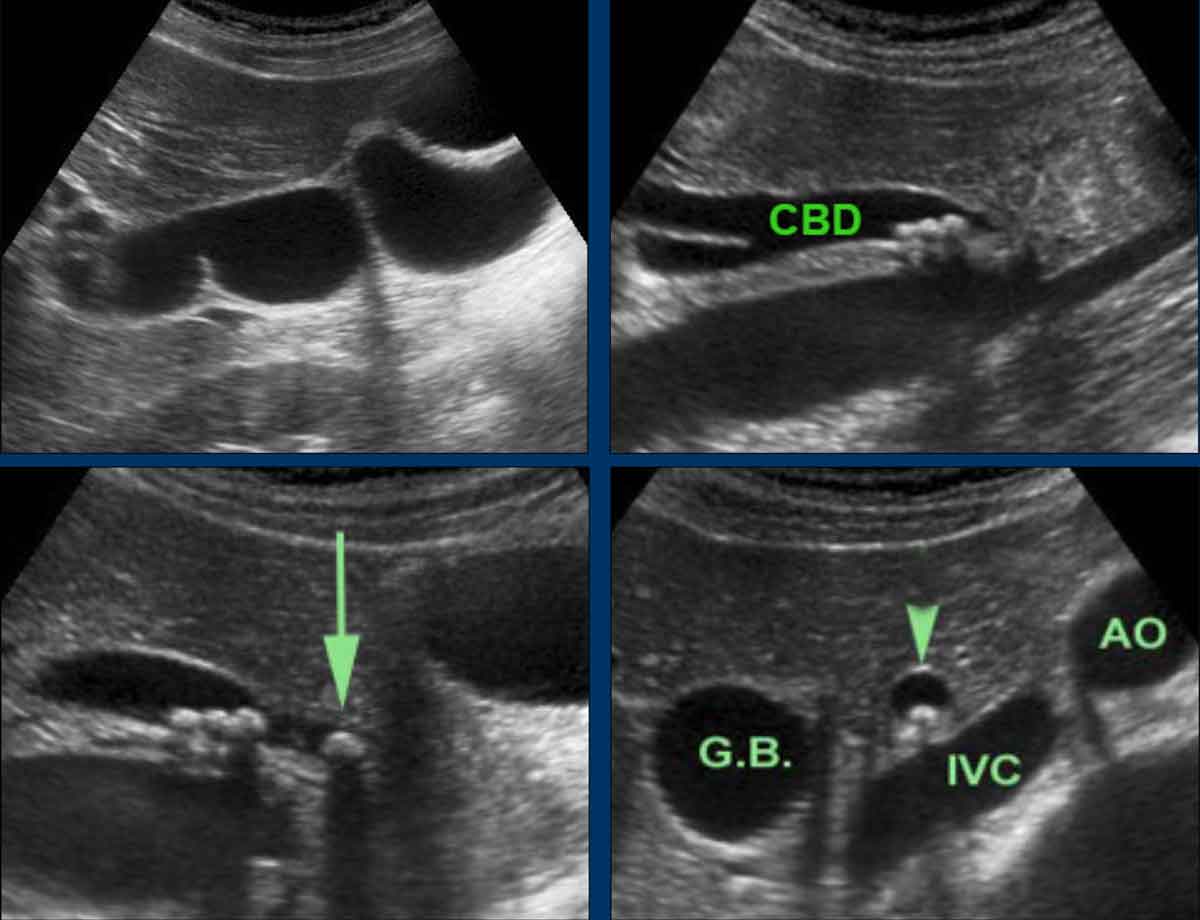
In the decubitus position, the pancreatic head and CBD (black arrow) are located anterior to the inferior vena cava (IVC).
Despite their retroperitoneal position, the pancreatic head, including the CBD (yellow arrow), may shift markedly to the left—a finding particularly notable in women.
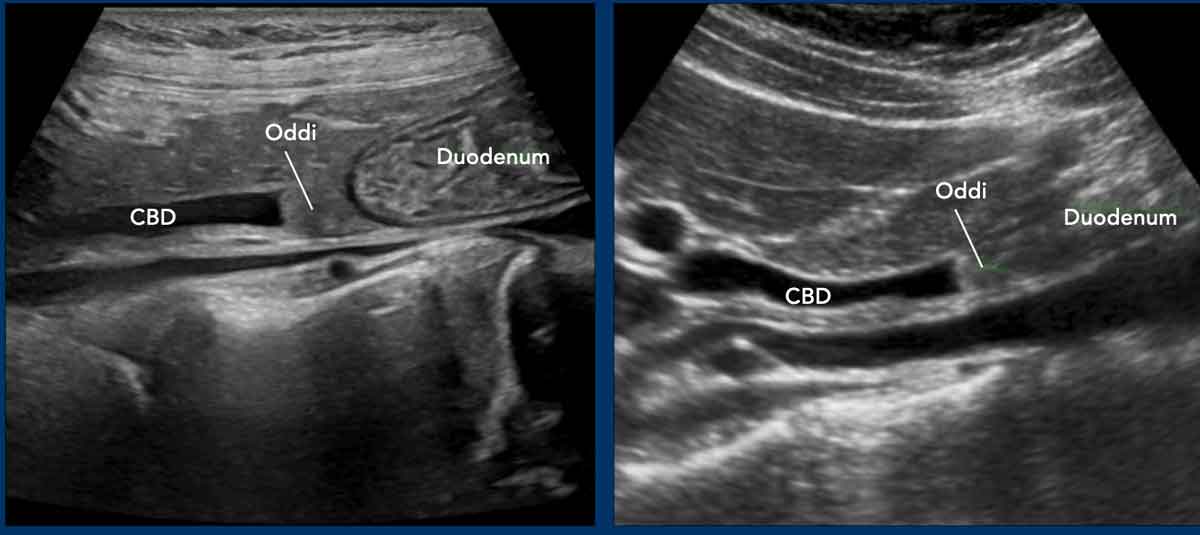
The normal distal CBD may have a blunt ending, which is due to the contracted sphincter of Oddi (appearing as a greyish mass between the CBD and the duodenum).
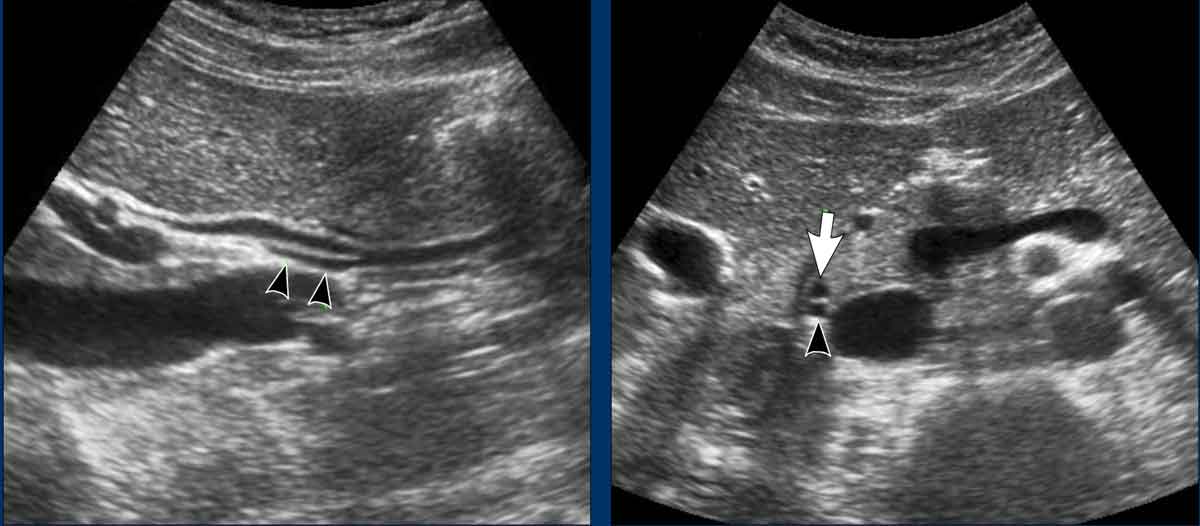
Cystic duct
The distal cystic duct can sometimes be visualized, entering the CBD.
In such a case the most distal part of the cystic duct (backl arrowheads) runs parallel to the CBD (white arrow), and is always located dorsally
Normal diameter of the CBD
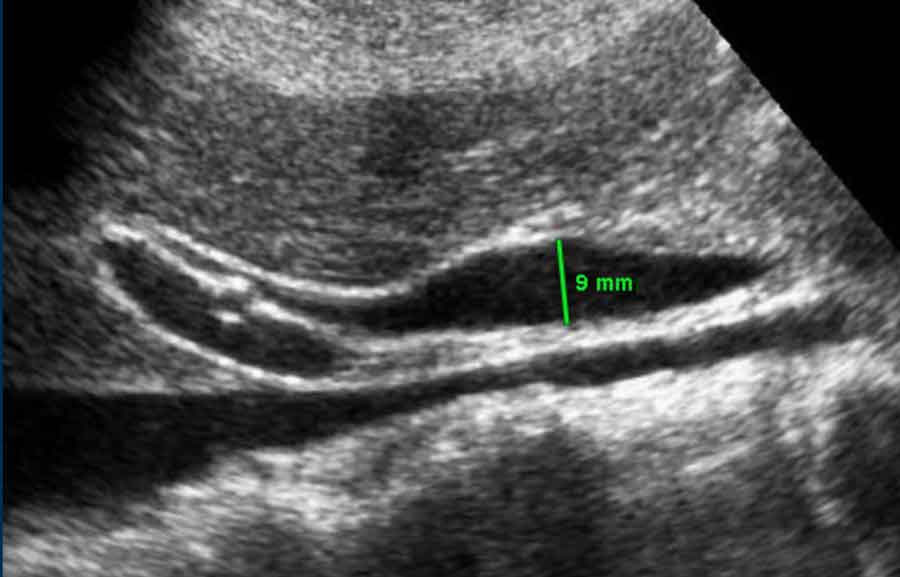
The diameter of the CBD varies with the patient’s age and position.
While the extrahepatic CBD can be quite wide, a tapering appearance in both the proximal and distal directions suggests low intraluminal pressure and, therefore, the absence of actual obstruction (see figure).
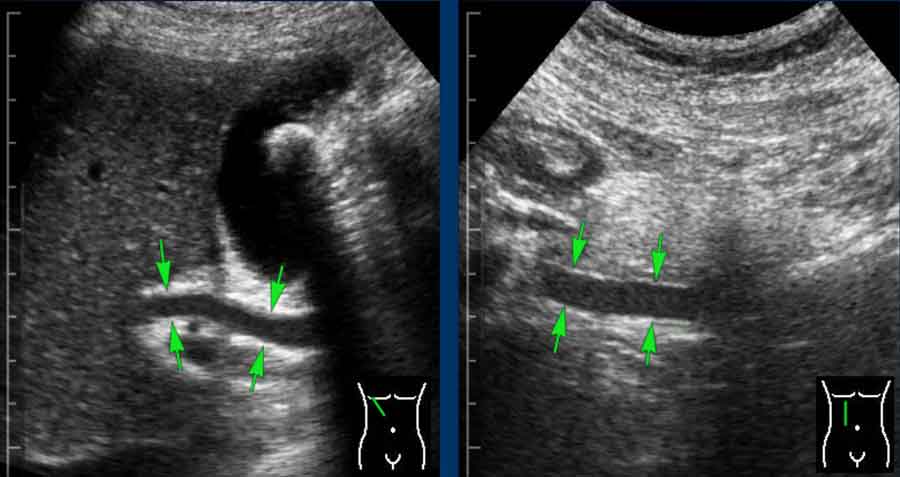
Dilatation of the CBD
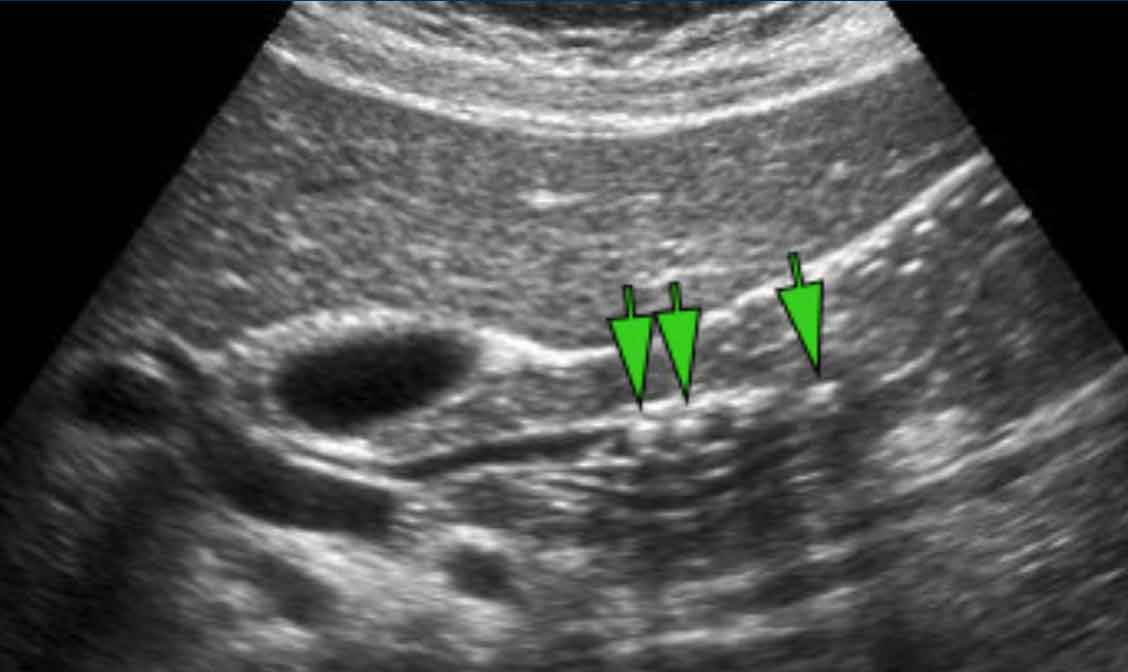
If the CBD (arrows) does not taper proximally nor distally, this is very suggestive for actual distal CBD obstruction (although the obstructing stone itself is often not visible)
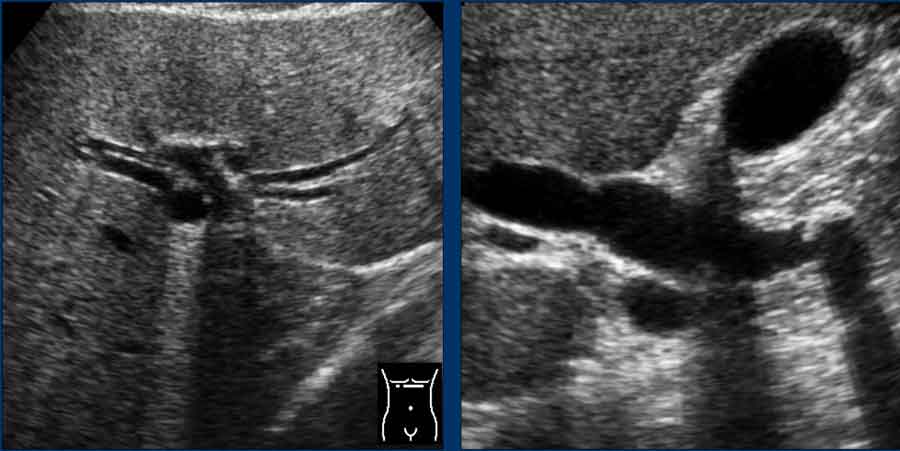
Widening of the intrahepatic CBD diameter, in combination with peripherally located "tramlines," strongly suggests actual CBD obstruction.
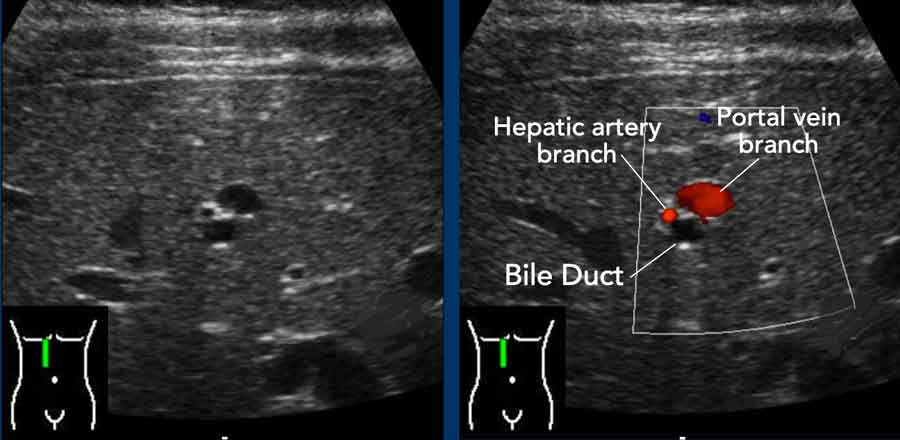
Detail of a dilated left hepatic duct , accompanied by a portal vein branch and a hepatic artery branch, as demonstrated by Color Doppler
Common Bile Duct Stones
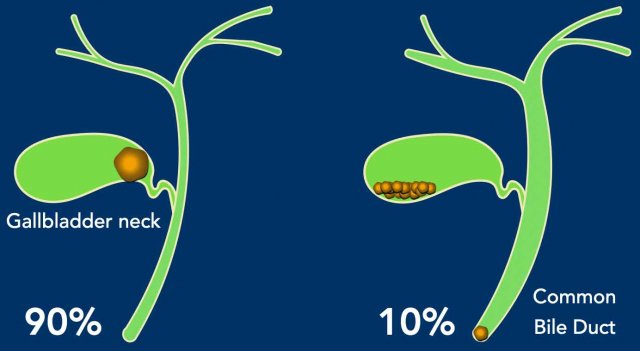
Of all patients presenting to the ER with biliary colic, the vast majority (approximately 90%) have a stone obstructing the gallbladder. Only about 10% of cases are due to a common bile duct (CBD) stone.
A CBD stone is significantly more dangerous than a gallbladder stone, as it can lead to serious complications such as:
- Cholangitis with septicaemia
- Liver abscesses
- Biliary pancreatitis
ERCP is required for stone removal, but carries intrinsic risks, including perforation and pancreatitis, and is associated with a much higher mortality rate.
Management
Patients with CBD stones should be referred urgently for endoscopic stone removal, followed by cholecystectomy to prevent further migration of stones from the gallbladder to the CBD.
The colicky pain, experienced by the patient, is identical to that of an uncomplicated biliary colic.
However, after 6–12 hours, the following manifestations typically occur:
- Dark urine
- Pale (acholic) stools
- Cholestatic laboratory findings
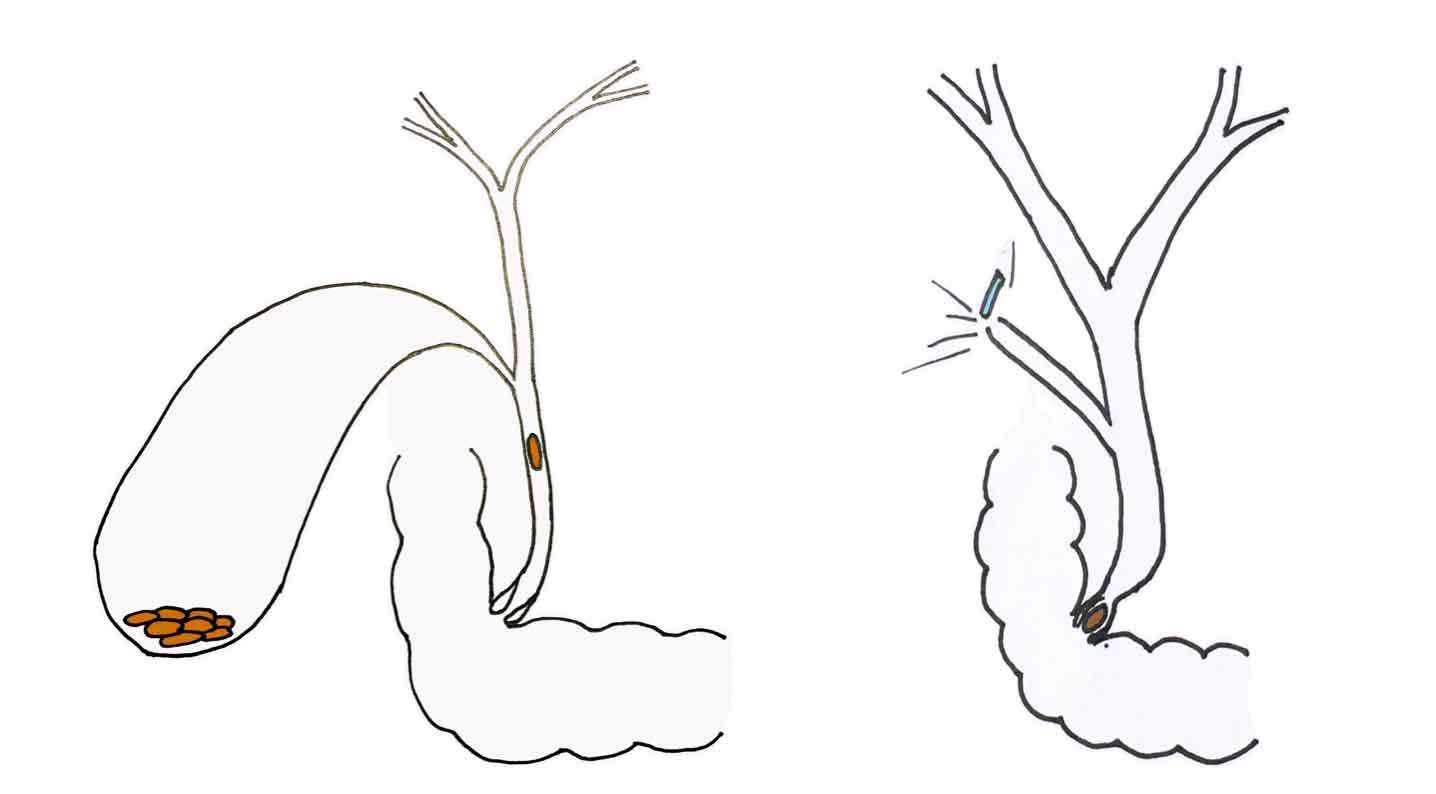
Most common bile duct stones originate from gallstones that migrate from the gallbladder to the CBD during a colic episode. These are usually small stones.
In elderly patients, particularly long after cholecystectomy, stones may also form de novo within a dilated CBD.
Case 1
37-year-old female presented with sudden onset of severe epigastric pain at 02:00 AM.
Emergency Department Course:
- Arrived at the ER at 03:00 AM.
- Initial laboratory investigations were unremarkable.
- Pain resolved promptly following administration of spasmolytics.
- Abdominal ultrasound performed at 08:00 AM.
First look at the US images and describe the findings.
Then continue reading...
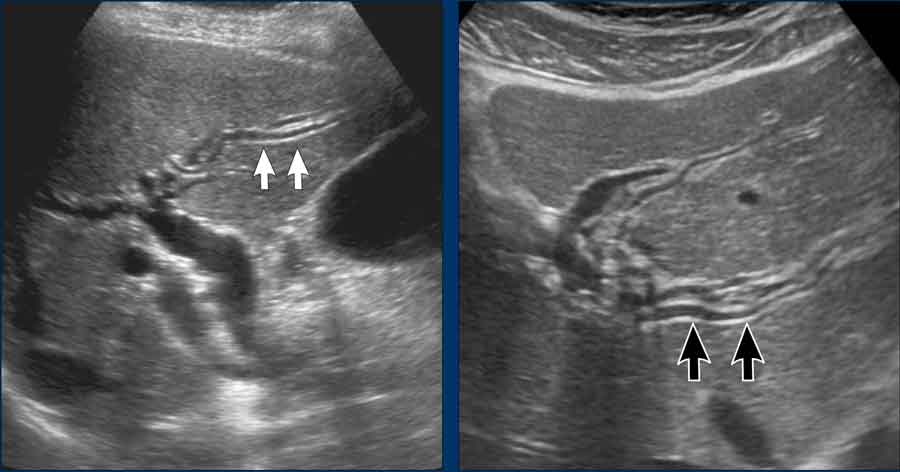
US findings
- Contracted gallbladder with small stones and reperfusion edema of the wall (“silent witness” of the colic, due to temporary ischemia during hydrops)
- Normal CBD (arrows). Note the cystic duct (arrowheads) entering the CBD from dorsally.
Management Plan
Elective cholecystectomy scheduled within 10 days.
Continue...
Subsequent Course
- The patient presented to the ER on two further occasions with episodes of colicky abdominal pain.
- Laboratory findings remained within normal limits on both visits.
- Pain resolved with medical management each time.
Current Presentation
- Now presents again to the ER with colicky pain.
- New findings: Dark urine and cholestatic laboratory profile.
This means that we have to conclude that the stones must have passed to the CBD.
US findings
- The gallbladder now is normal.
- Multiple small stones in a dilated CBD
- The most distal CBD stone (arrow) is actually obstructing the lumen
- Note the rounded shape of the axial CBD (arrowhead), indicating high pressure.
The patient underwent a successful ERCP with sphincterotomy, followed three days later by a laparoscopic cholecystectomy.

Case 2 post ERCP pancreatitis
A 41-year-old female, an unfortunate companion case, presented with a similar history.
She underwent a successful ERCP with stone extraction.
However, one day later, she developed severe epigastric pain and was diagnosed with severe post-ERCP pancreatitis, requiring 6 weeks of hospitalization, including 2 weeks in the ICU.
Learning Points
- While ERCP is a valuable and often unavoidable procedure for the removal of common bile duct (CBD) stones, it remains high-risk, with a morbidity rate of 12% and a mortality rate of 0.2%.
- In patients with recurrent biliary colic, do not allow time for stones to migrate from the gallbladder to the CBD.
- If the diagnosis of symptomatic gallstone disease is confirmed, proceed with cholecystectomy as soon as possible (ASAP).
What to do ... If the colic is over?
If the colic is over or if colics are intermittent, then the question is:
- Did all stones pass to the duodenum?
- Or are there still stones in the CBD ?
This is extremely important, as performing a cholecystectomy while a stone remains in the CBD can lead to complications.
During a subsequent colic, surgical clips on the cystic duct may dislodge, potentially causing bile leakage and biliary peritonitis.
CBD stone detection
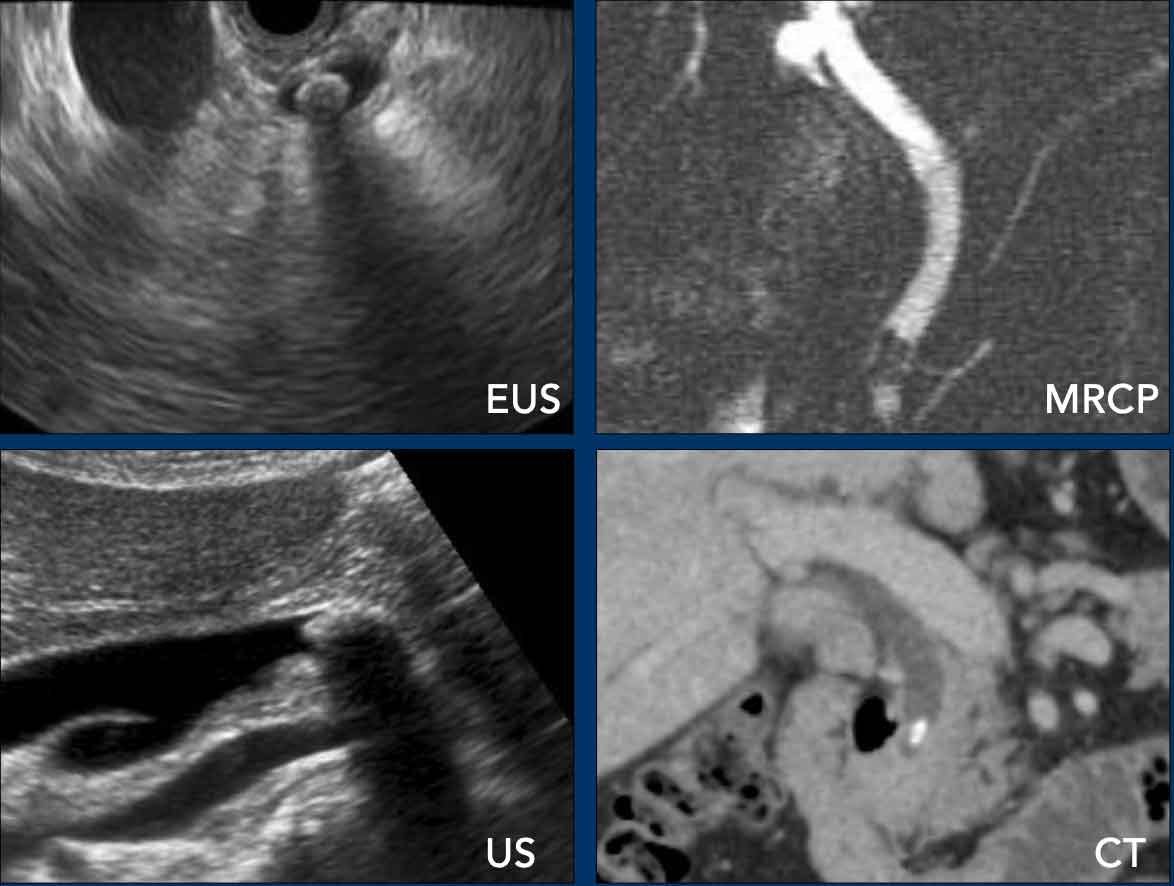
There are several methods for detecting residual stones in the common bile duct (CBD), but only endoscopic ultrasound (EUS) is sufficiently reliable to confirm CBD clearance prior to cholecystectomy.
- EUS is the most accurate imaging modality for both detecting and excluding CBD stones.
- MRCP is non-invasive but may miss small stones in up to 15% of cases.
- CT can sometimes identify CBD stones, yet it fails to detect small or isodense stones in approximately 50% of cases.
- Standard ultrasound may miss stones, as the distal CBD is often poorly visualized.
If any imaging modality identifies CBD stones, endoscopic removal is indicated.
Standard Abdominal Ultrasound
The overall detection rate of CBD stones using ultrasound (US) is generally low (<40%).
However, the diagnostic yield of US improves significantly during a biliary colic, as the bile ducts are typically dilated, making stone detection more reliable.
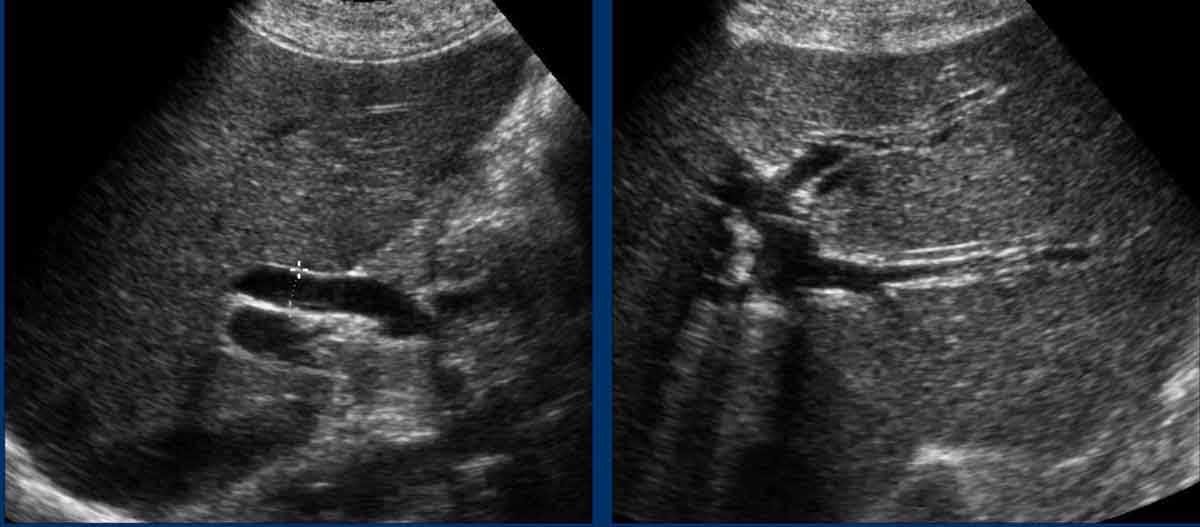
In this case, the ultrasound was performed during a colic, and both the dilated ducts and the stone are clearly visualized.
However, in daily practice, ultrasound is rarely performed during an active colicky attack.
Typically, patients have already received medication or are spontaneously pain-free by the time the ultrasound is performed.
This ultrasound was conducted after the colic. The multiple small stones (indicated by arrows) within a thin common bile duct are difficult to visualize.
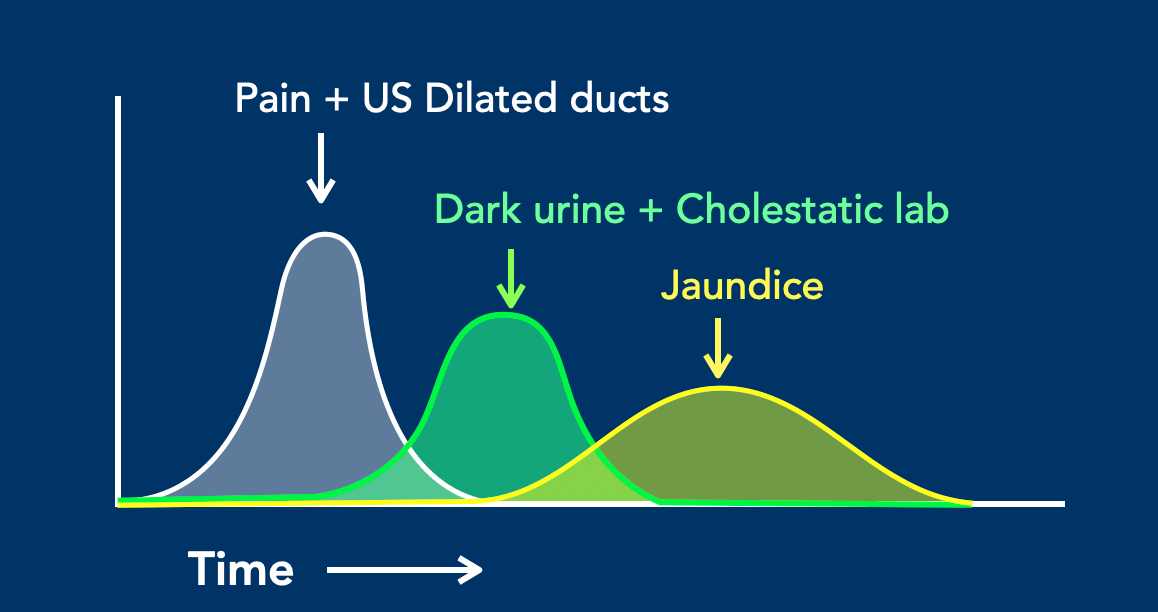
In a patient with biliary colic due to a common bile duct (CBD) stone, the clinical, laboratory and US findings depend on the timing of evaluation.
This graphic illustrates that while pain and bile duct dilatation occur immediately, dark urine and cholestatic laboratory abnormalities appear later, typically after 6–12 hours. By this time, the pain and bile duct dilatation may have already resolved.
Jaundice develops even later and also resolves more slowly.
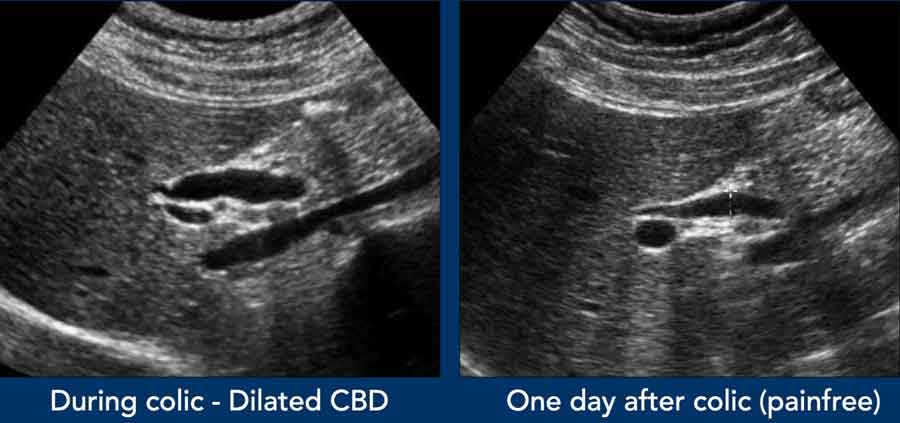
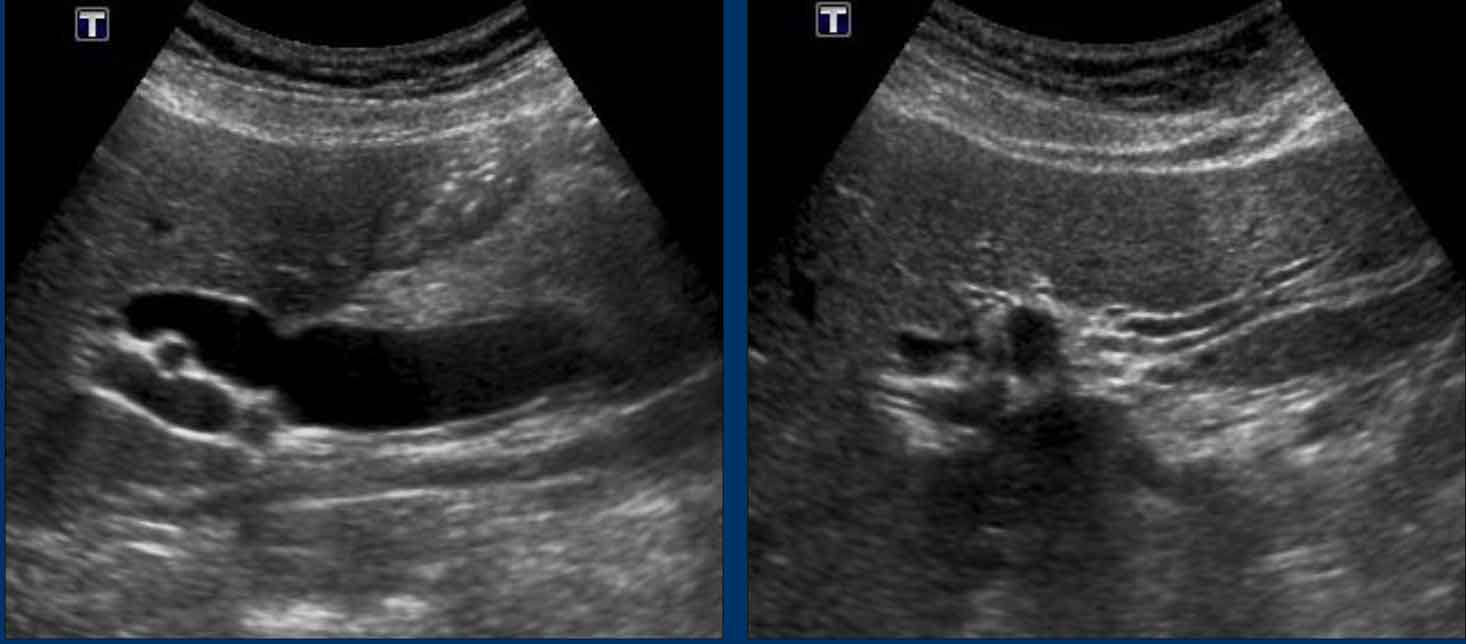
This patient presented with biliary colic and underwent ultrasound imaging.
At that time, the CBD was dilated, but laboratory tests and urinalysis were unremarkable.
The following day, the patient was asymptomatic, yet cholestatic liver enzymes were significantly elevated, and the urine was dark brown. Notably, the CBD was no longer dilated.
Thus, the timing of the examination is critical. A non-dilated CBD does not exclude the presence of a CBD stone.
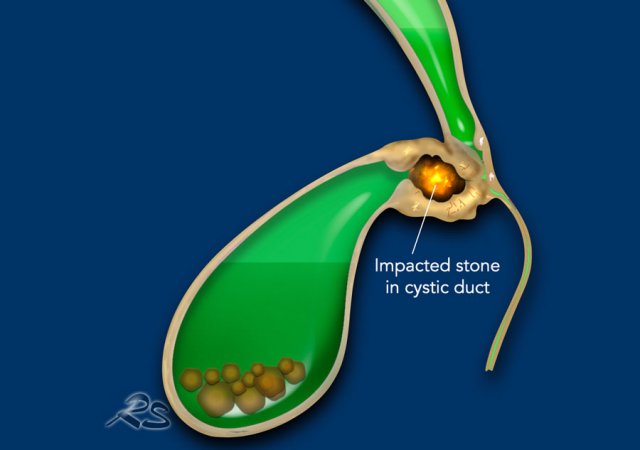
What is the appearance of the gallbladder after a CBD colic?
After a CBD colic, the gallbladder may exhibit specific findings.
Initially, a stone may become impacted in the cystic duct, leading to gallbladder hydrops and temporary ischemia.
Once the stone passes into the CBD and the obstruction resolves, the gallbladder may display characteristic post-colic changes, often referred to as "silent witnesses":
- Reperfusion edema
- Hyperemia
- Biliary sludge
- Post-colic contraction (sometimes described as "after-labour" contraction)
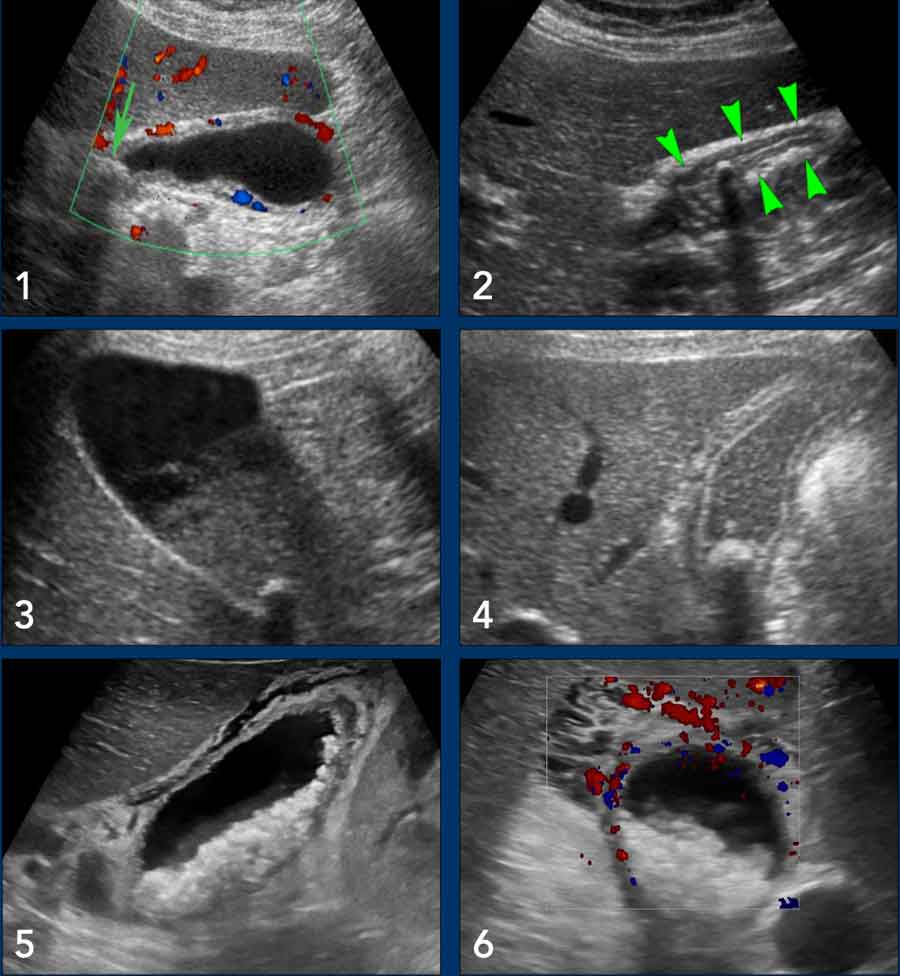
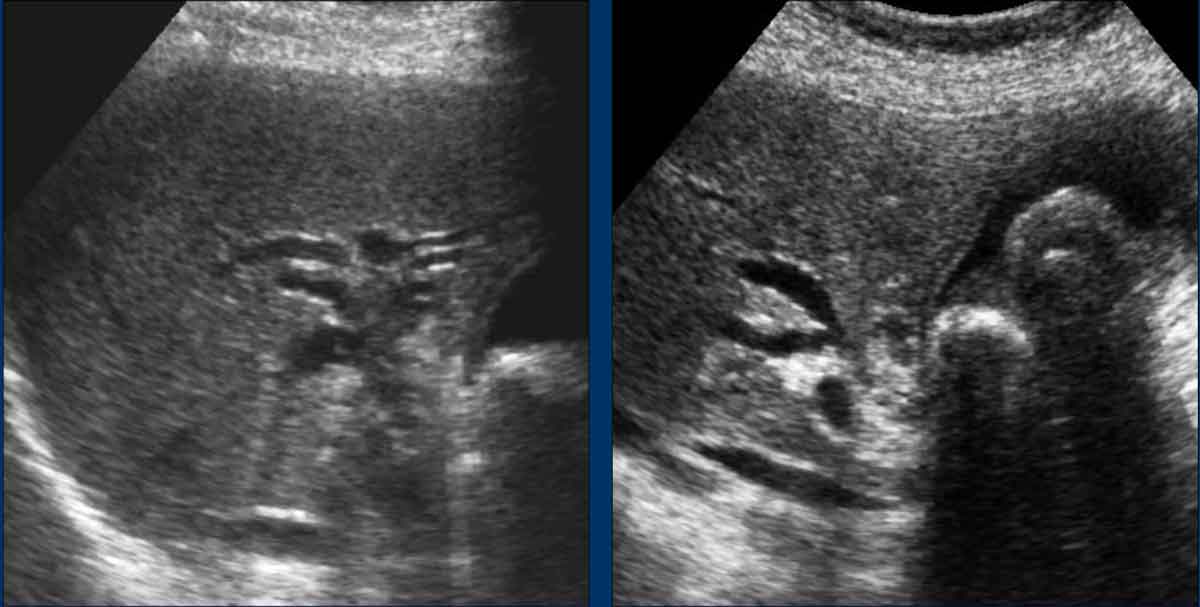
Examples
- Reperfusion edema and hyperemia
- Post-colic contraction
- Sludge
- Reperfusion edema
- Extreme reperfusion edema
- Same patient. Notice hyperemia.
Notice that some of these examples resemble US-findings of a cholecystitis.
However all these patients were painfree and had a normal CRP.
Edema and hyperemia quickly resolved.
Acute cholangitis
Acute cholangitis due to a common bile duct stone is primarily a clinical diagnosis.
Typically, the patient presents as severely ill, with a history of biliary colic and signs of septicemia, accompanied by:
- Cholestatic laboratory findings
- Markedly elevated CRP and leukocytosis (↑↑↑)
However, in elderly patients, classic signs such as fever or leukocytosis may be absent.
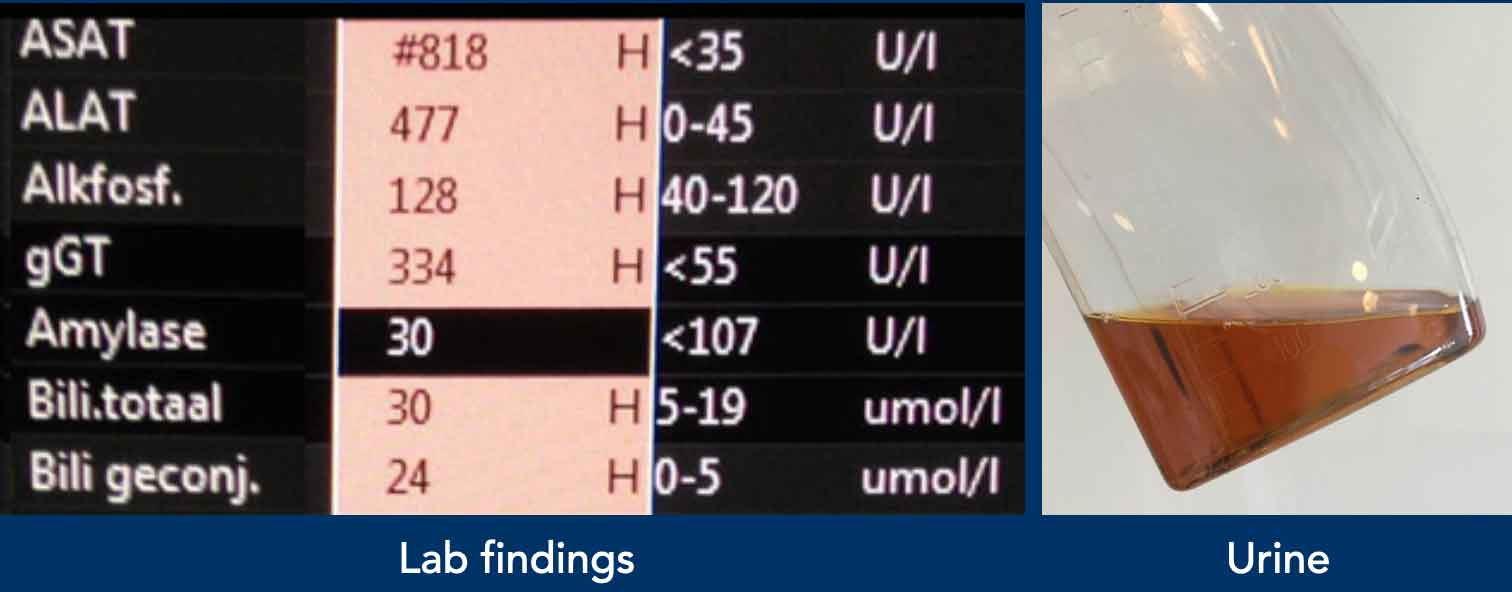
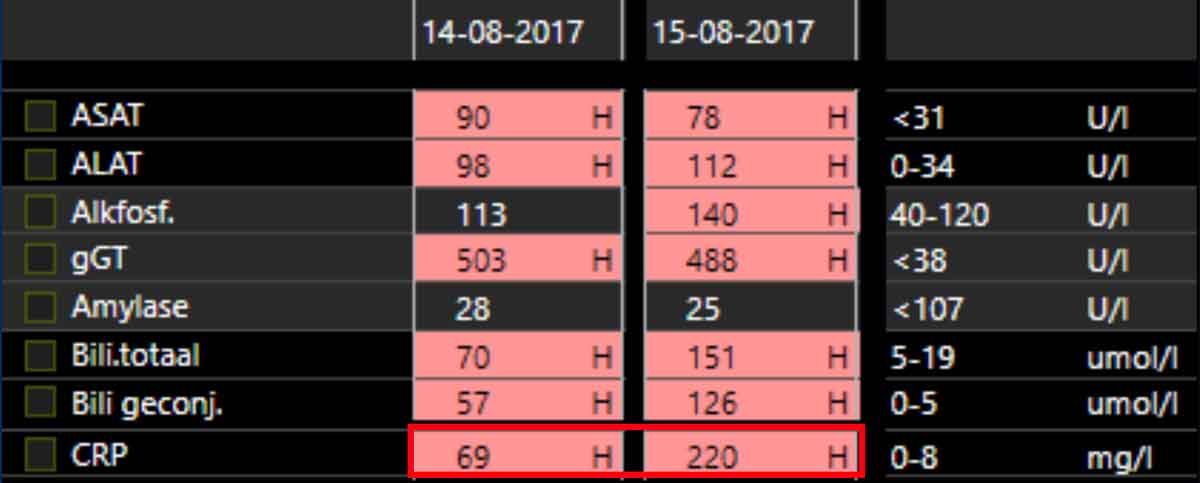
Image
Note that all laboratory values—except amylase (excluding pancreatitis)—are abnormal.
Additionally, there is a dramatic rise in CRP within 24 hours.
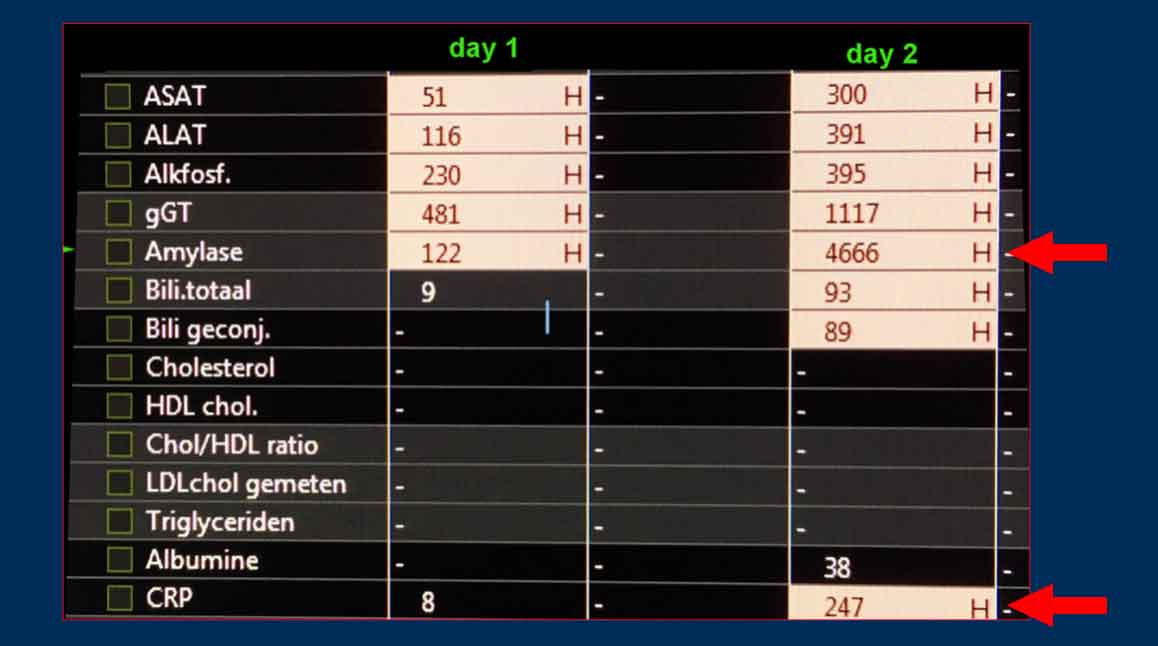
Biliary Pancreatitis
Biliary pancreatitis is also basically a clinical diagnosis.
These lab findings are of a severely painful patient with:
- Elevated lipase/amylase (suggestive of pancreatitis)
- Cholestatic laboratory findings
- Rapidly rising CRP (indicating a significant inflammatory response)
Dilated CBD without complaints or cholestatic lab
In some patients, a dilated common bile duct and even dilated intrahepatic bile ducts may be incidentally detected in the absence of clinical symptoms or cholestatic laboratory abnormalities.
In such cases, the following differential diagnoses should be considered:
- Post-cholecystectomy state (the CBD may assume a compensatory reservoir function over time).
- Chronic opiate use (e.g., methadone, oxycodone, fentanyl), which can induce sphincter of Oddi dysfunction (SOD) due to chronic spasm.
- Duodenal diverticulum (present in ~15% of the population; periampullary diverticula are specifically associated with CBD dilation).
85-year-old female with an incidental finding 45 years post-cholecystectomy.
Ultrasound
Dilated common bile duct and intrahepatic bile ducts.
Normal liver function tests and no clinical symptoms.
Incidental finding in a 58-year-old male during hepatitis B screening.
No symptoms, normal liver enzymes.
Ultrasound
Dilated common bile duct and intrahepatic bile ducts.
History: Chronic methadone use for 10 years.
Wide CBD and Periampullary diverticulum
Periampullary duodenal diverticula are found in 15% of the population, and are associated with a wide CBD.
- If actively looked for, air-filled diverticula can be visualized on ultrasound (arrowheads).
- For gastroenterologists performing ERCP, their presence may predict difficult cannulation of the papilla, increasing the risk of complications.
- Additionally, these patients have a higher likelihood of developing CBD stones.
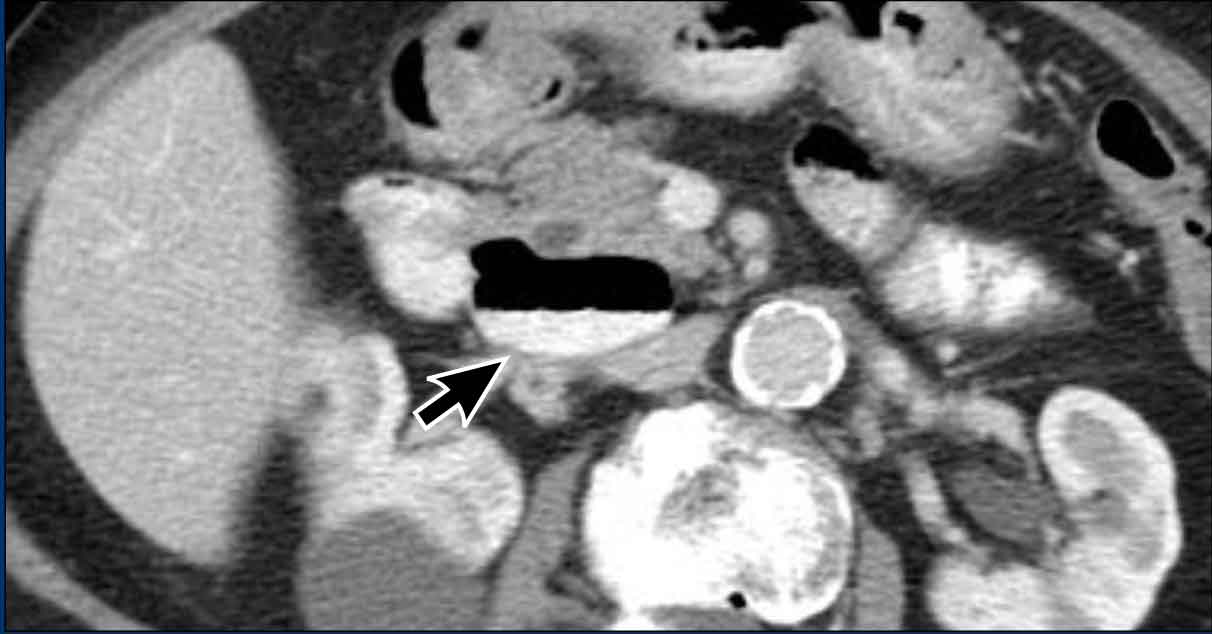
CT scan of a patient with a duodenal diverticulum (arrow).
Mirrizzi syndrome
Described by Pablo Mirizzi, an Argentinian surgeon, in 1948.
It is a rare complication of gallstone disease in which a stone becomes impacted in the cystic duct or the neck of the gallbladder, causing external compression of the common hepatic duct or common bile duct.
This compression leads to obstructive jaundice and can mimic other biliary conditions, such as cholangiocarcinoma or pancreatic cancer.
Clinical presentation
A 64-year-old female presents with a 3-week history of upper abdominal pain, now accompanied by jaundice.
Laboratory findings reveal a cholestatic pattern (elevated alkaline phosphatase, gamma-glutamyl transferase, and bilirubin) and an elevated CRP of 25 mg/L.
Ultrasound revealed intrahepatic bile duct dilatation and a thick-walled gallbladder with stones. The CBD could not be visualized.
Differential Diagnosis based on US findings
- Mirizzi Syndrome: Gallstone in cystic duct/gallbladder neck compressing the common hepatic duct.
- Choledocholithiasis: Obstructing stone in the common bile duct.
- Cholangiocarcinoma: Bile duct cancer (less likely without a history of pain or weight loss).
- Pancreatic head cancer: Can cause painless jaundice but often has weight loss and a visible mass.
- Acute cholangitis: unlikely in view of CRP 25 and absence of fever.
- Gallbladder cancer: Less likely because there is no mass.
Continue with the CT...

The distal CBD has a normal caliber up tp the level of an impacted stone in the gallbladder neck or cystic duct, which is surrounded by inflammation.