TAVI / TAVR
Measurements, access route and complications
Richard Takx¹, Jan Baan¹ and Csilla Celeng²
¹University Medical Center Amsterdam, ²UMC Utrecht, the Netherlands
Publicationdate
Severe aortic stenosis increases left ventricular afterload and workload, resulting in high mortality after symptom onset.
Transcatheter aortic valve implantation or replacement (TAVI/TAVR) is a key treatment option, with procedural success reliant on pre-procedural planning CT.
This article addresses:
- Annulus sizing for optimal valve selection.
- Vascular access to determine the best delivery route.
- High-risk anatomy, including low coronary ostia, heavy LVOT calcification, or unfavorable aortic angulation.
- Complications of TAVI
Introduction
TAVI - term used in Europe - and TAVR - a term used in USA, are essentially the same procedure.
TAVI and TAVR refer to the minimally invasive replacement of a diseased aortic valve using a catheter-based approach and have revolutionized the management of aorta stenosis (AS), becoming the standard of care
for patients across a wide spectrum of surgical risk.
Procedural success depends largely
on precise pre-operative planning.
While echocardiography confirms the
diagnosis, it cannot provide the 3D spatial resolution required for device
sizing, procedural safety and vascular access. Consequently, a dedicated
planning CT is required for pre-procedural assessment.
The radiologist plays an important role within the structural heart team. Specifically, the radiologist should:
- Provide accurate annulus size, to determine optimal valve size, minimizing the risks of paravalvular leak or annular rupture.
- Determine the vascular access route, identifying the optimal delivery approach (iliofemoral vs. alternative access), while also taking into account vessel tortuosity or calcification.
- Identify high-risk anatomical features, such as low coronary ostia, heavy calcification of the left ventricular outflow tract (LVOT), or specific aortic angulations (e.g., a horizontal aorta with an angle ≥49° between the horizontal plane and the aortic annulus, measured in a coronal view).
Video
Severe calcified aortic stenosis treated with inserting a bioprosthetic valve and deploying it within the native aortic valve, which is pushed aside.
CT protocol for TAVI
CT protocol for TAVI includes
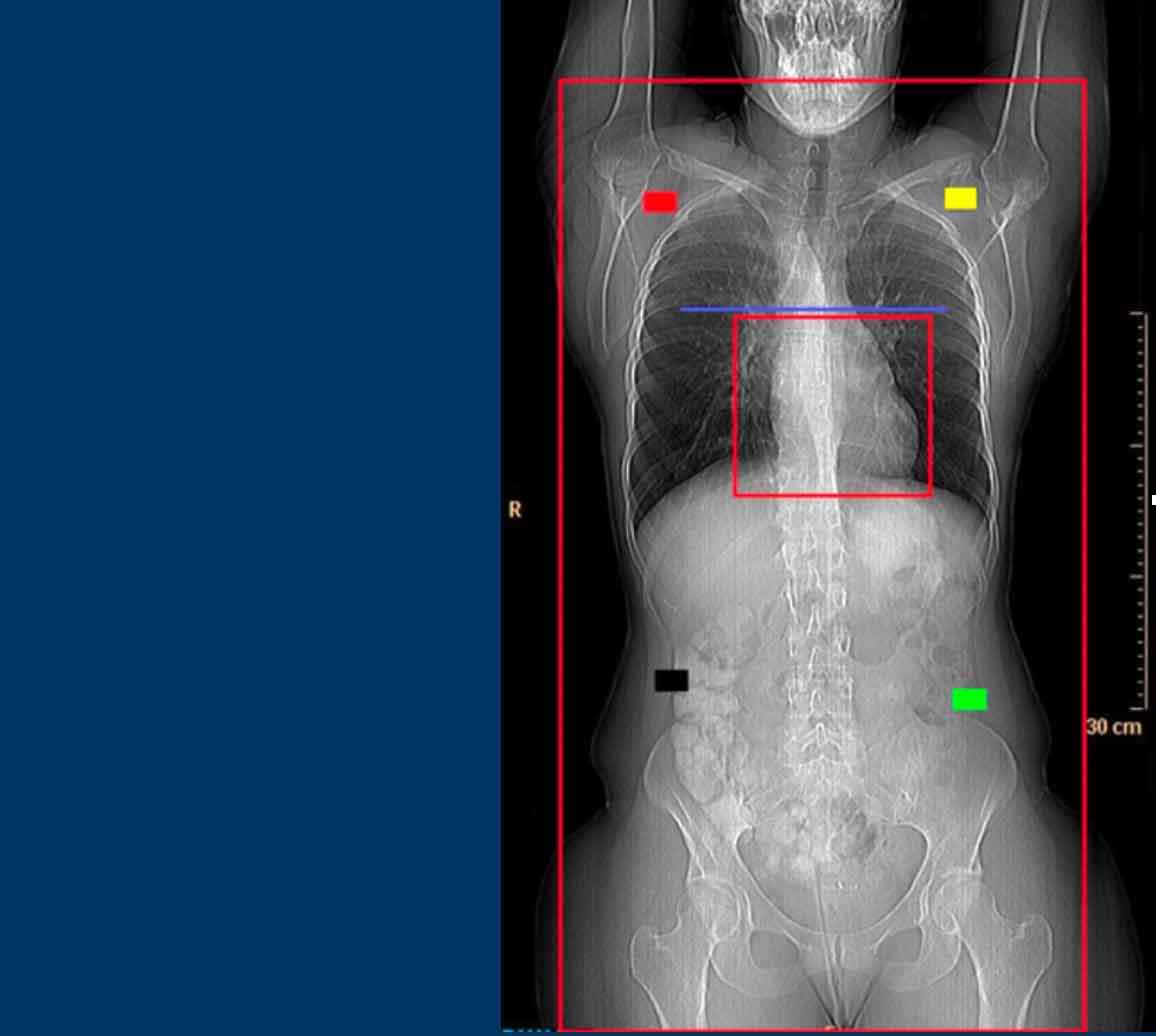
- Topogram
- Scan range must include the subclavian arteries down to the lesser trochanters
- Non-contrast Cardiac CT
- optional, but highly recommended to determine the severity and distribution of aortic valve calcification.
- Contrast-enhanced Cardiac CT
- Utilizes retrospective ECG-gating or prospective ECG-triggering in systole with wide padding to capture the aortic valve in systole when the annulus is at its maximum dimension.
- No nitroglycerin or beta-blockers should be administered.
- Contrast protocol
- Requires high iodine concentration (350–400 mgI/mL) injected at a high flow rate of 4–5 mL/s.
- Body Flash CTA scan
- Evaluates the vascular access route and performed immediately after the cardiac CT without requiring an additional contrast bolus.
Aortic valve calcium score
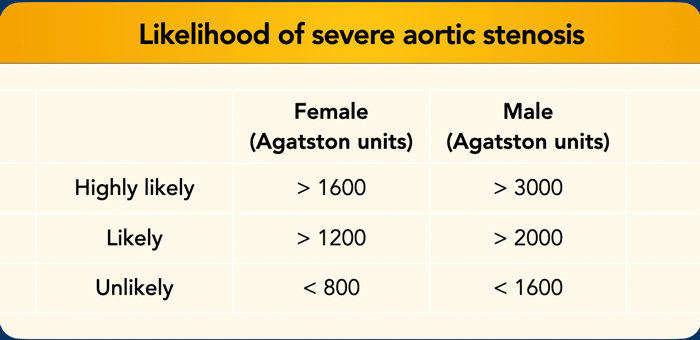
Sex specific cutoffs to determine the likelihood of severe AS based on Agatston scores (adapted from: (2).
Please note that females develop severe aortic stenosis with less total valvular calcification, more fibrosis, and distinct anatomical and hemodynamic profiles than males.
Therefore, applying a lower calcium threshold (>1200 Agatston units) is essential to ensure accurate diagnosis and prevent underdiagnosis.
Table
Sex specific cutoffs to determine the likelihood of severe AS based on Agatston scores.
Guidelines of the European Society of Cardiology, American Heart Association and American College of Cardiology designate transthoracic echocardiography (TTE) as the first-line modality for AS assessment.
However, discordant results—particularly in low-flow, low-gradient AS—may occur.
In such cases, a gated non-contrast cardiac CT helps differentiate true severe AS (TAVI-indicated) from pseudo-severe AS by quantifying the calcification burden.
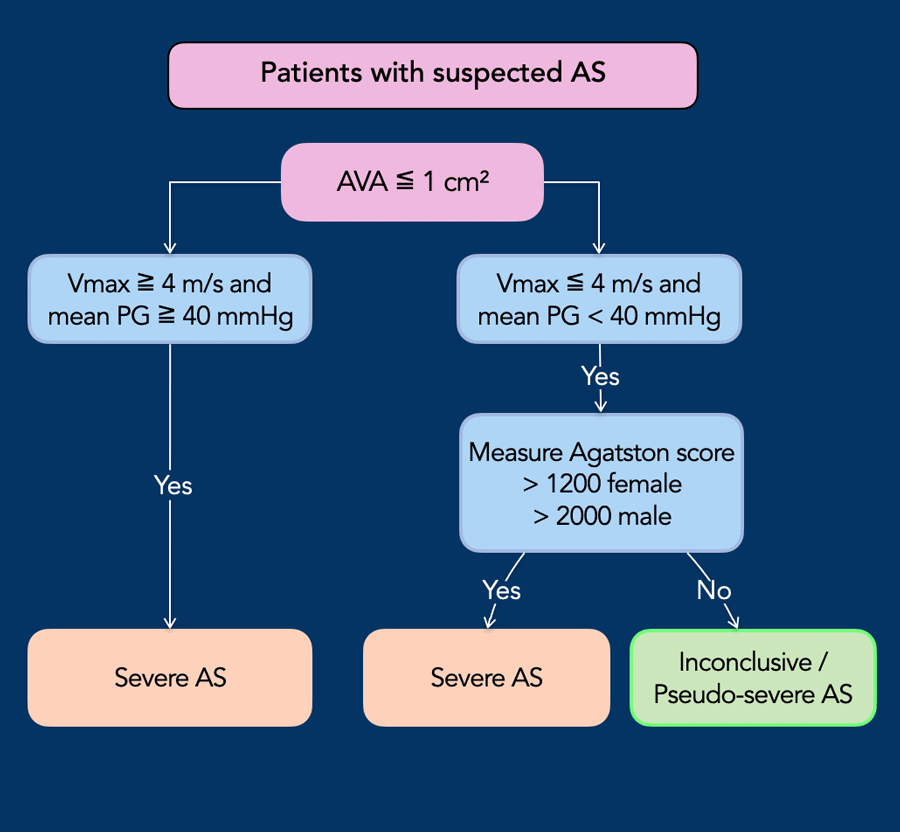
Flow chart
Modified flow chart based on (2).
High-gradient AS is diagnosed via echocardiography.
Non-contrast CT
calcium scoring is crucial for resolving indeterminate low-flow, low-gradient
cases (AVA ≤ 1 cm², Vmax ≤ 4 m/s, mean PG < 40 mmHg).
Severe AS is confirmed by a score >
1200 in females or > 2000 in males.
Lower scores indicate pseudo-severe AS,
where poor valve opening is secondary to low stroke volume rather than
anatomical stenosis.
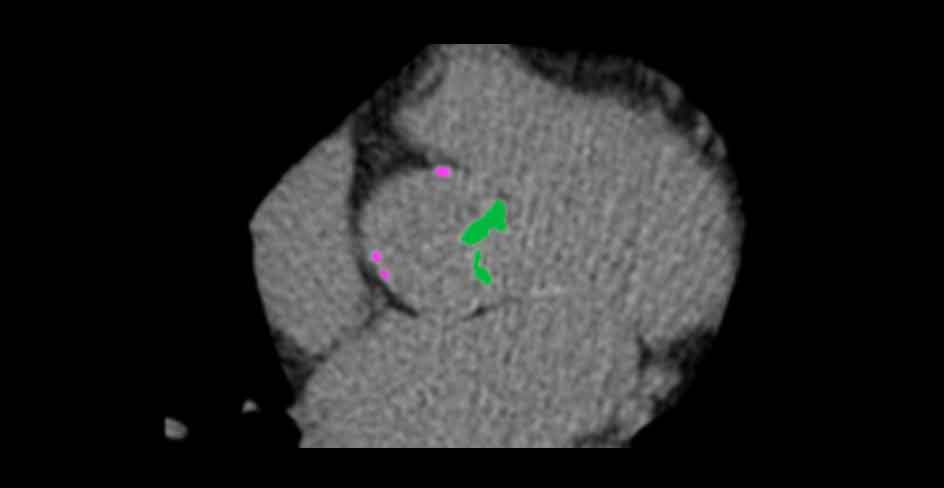
Example
A female patient with Agatston score 2480.
This makes severe aortic stenosis highly likely.
Aortic annulus size
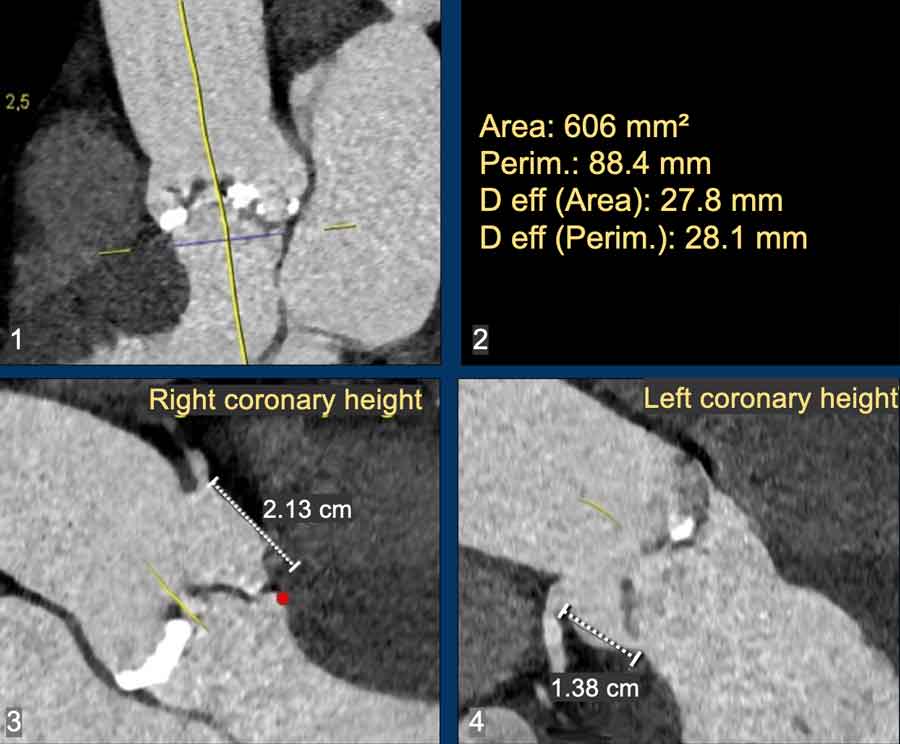
Accurate aortic annulus sizing is essential in TAVI to avoid complications:
- Undersizing (Valve too small) → Risk of paravalvular leak or valve embolization/migration.
- Over-sizing (Valve too large) →Risk of annular rupture or compression of the conduction system beneath the membranous septum, causing a high-degree heart block (frequently requiring a permanent pacemaker).
CT is the gold standard for sizing:
- Measurements (area/perimeter) are taken in systole (20–40% of the cardiac cycle), when the annulus reaches its largest dimensions. This ensures an optimal circumferential seal and prevents malpositioning.
Two other key CT assessments:
- Coronary artery height: the perpendicular distance from the annular plane to the coronary ostia (ideally >10–12 mm). If critically short, displaced native leaflets may block coronary flow.
- C-arm angulation: predicts the fluoroscopic angles for the intervention.
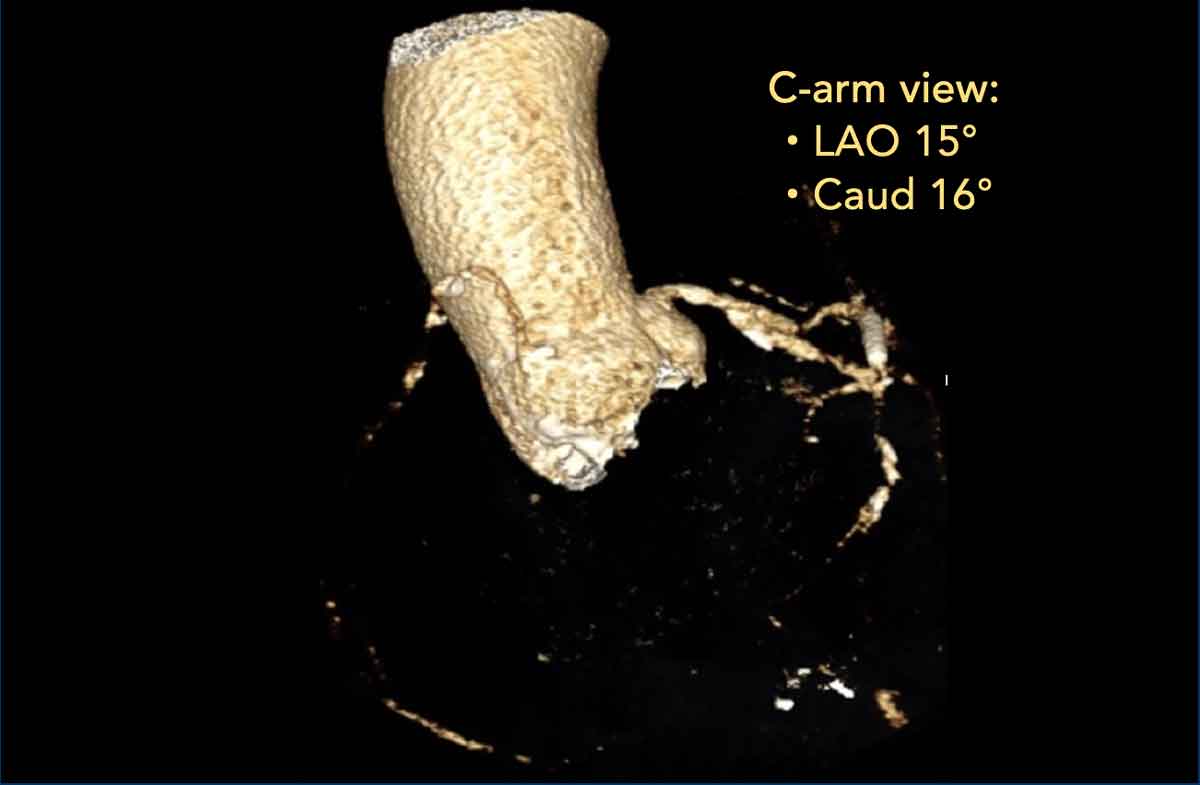
C-arm angulation
CT determines the ideal fluoroscopic deployment angles, prediciting for
both the traditional "3-cusp
coplanar view" (all
cusps aligned in a straight line) and contemporary “cusp-overlay views” (separating
the non-coronary cusp to optimize deployment depth).
This allows for
precise valve deployment, reducing time , radiation exposure and contrast
compared to trial-and-error angiography.
Bicuspid aortic valve
 Reference 3
Reference 3
Historically, a bicuspid aortic valve was considered a contraindication
for TAVI due to unique anatomical challenges, including asymmetric
calcification, elliptical annular geometry, and concomitant aortopathy.
Today, with advancements in imaging and newer generation valves, TAVI is
frequently performed in these patients, though the approach is highly
customized.
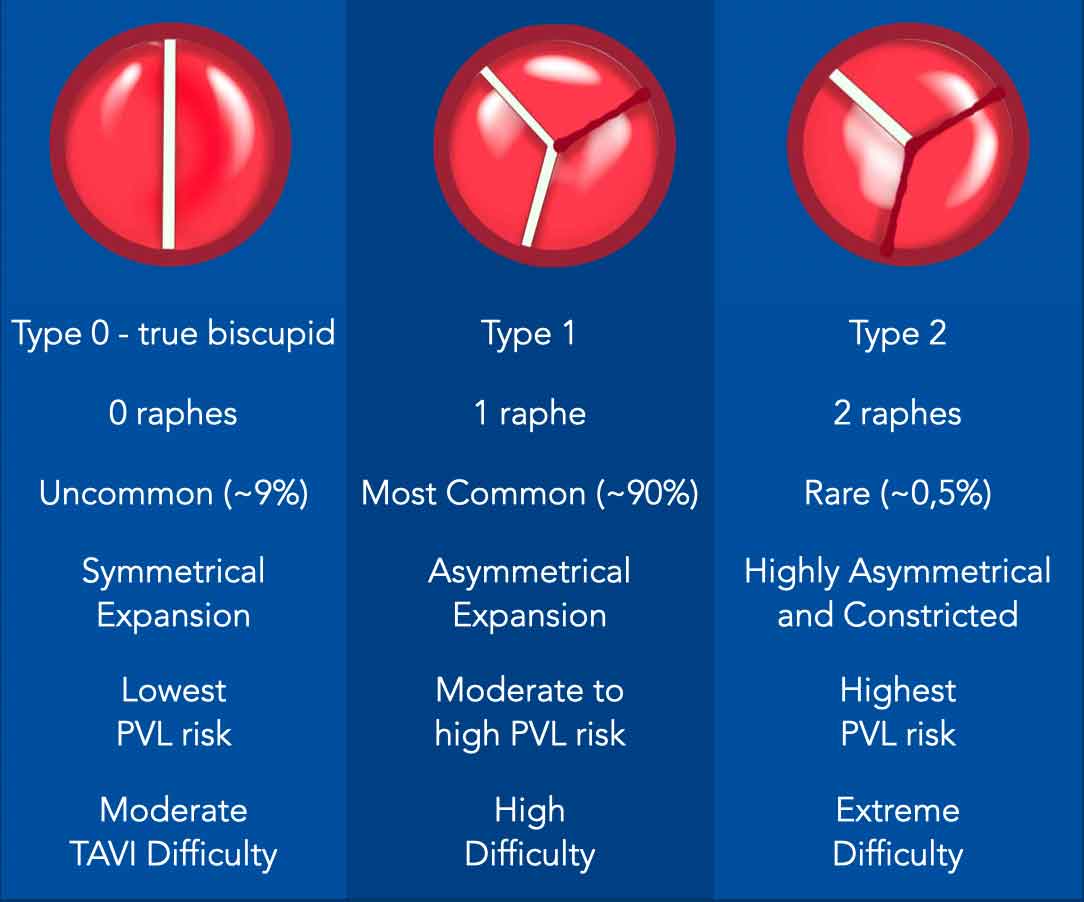
The Sievers Classification is widely utilized to categorize BAV
morphology based on the number of fused cusps (commissures) and the presence of
a raphe (congenital fusion line):
Type 0
- True bicuspid valve with two equally sized cusps and no raphe.
- Often functionally normal, but may develop premature calcific stenosis or regurgitation.
Type 1
- Most common type.
- Fusion of two valves (most frequently the Right and Left Coronary Cusps).
- One raphe - fibrous ridge or fusion line where two of the three normal aortic valve cusps have abnormally fused together during development.
Type 2
- Two raphes
- Severely altered architectural profile.
- Rare, but associated with more severe disease (e.g., earlier valve degeneration, higher risk of aortic dissection).
Supra-Annular Sizing
In classic trileaflet aortic stenosis, valve sizing is strictly dictated
by the dimensions of the virtual basal annular plane.
In BAV, however the most
restrictive, tightest part of the aortic
root anatomy is frequently located supra-annulary, at the level of the calcified
leaflets, raphe, or commissures.
The size of the valve is usually based on the supra-annular (4 to 5 mm
superior to the annulus) inter-commissural distance to prevent over-sizing and
annular rupture.
A projected circle can be used to determine the optimal valve size.
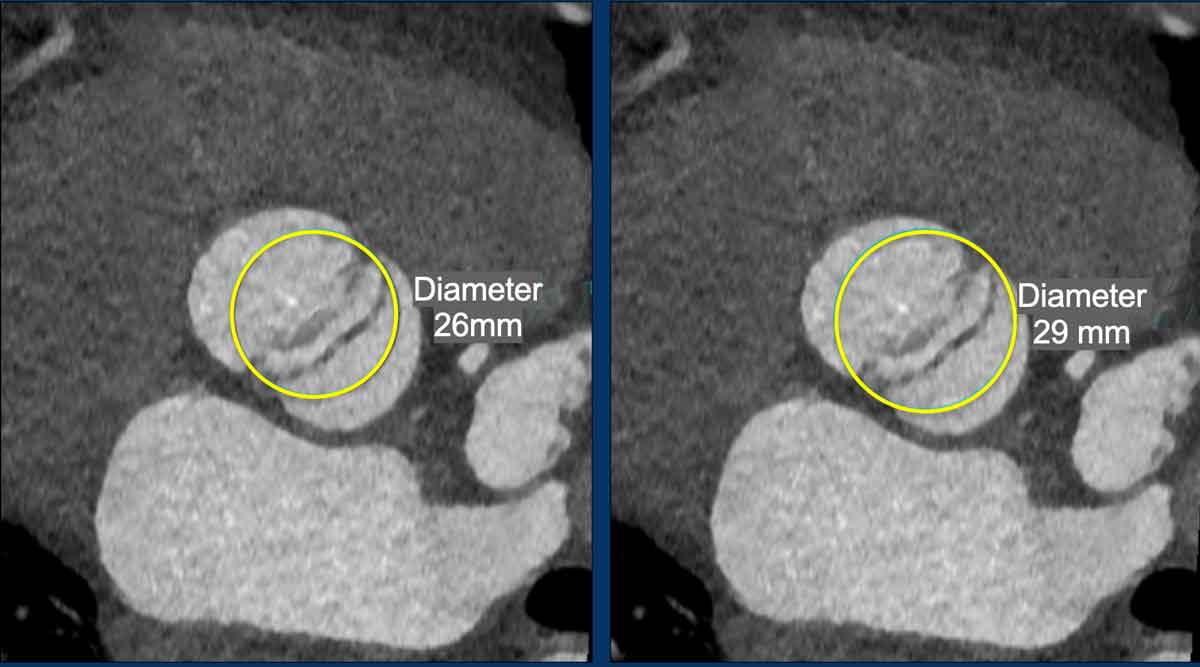
Example
75-year-old female with Type 1 BAV. Based on the projected circle a 29
mm Sapien 3 Ultra was successfully implanted without complications.
The CT image demonstrates, that a 26 mm valve would have resulted in
under-sizing and significant paravalvular leakage.
Transcatheter heart valves
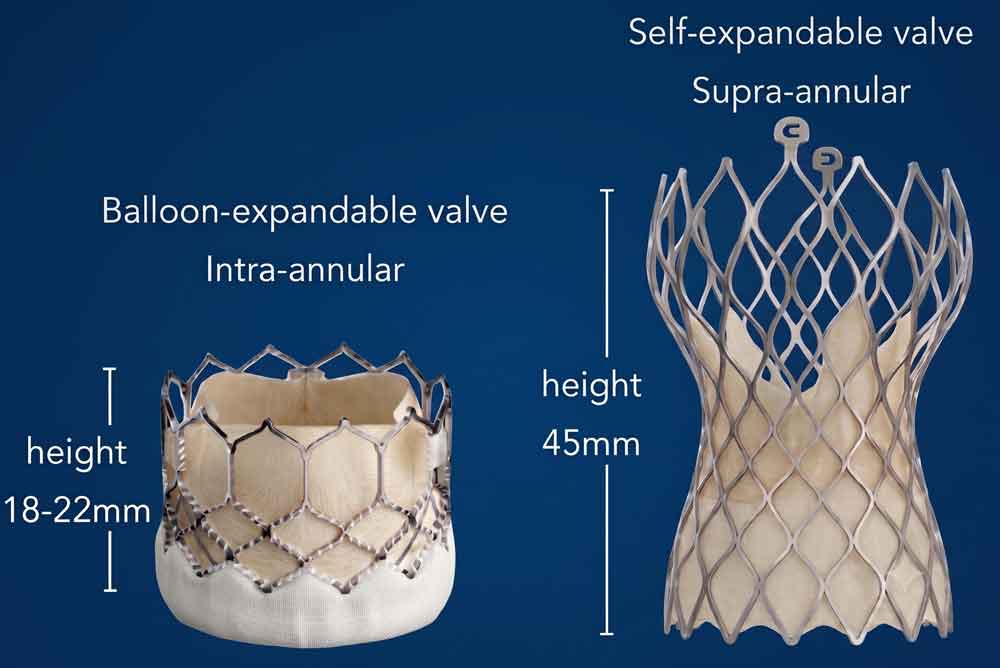
Balloon-expandable vs. Self-expanding
Operators must choose between:
- Balloon-expandable valves, which have higher radial strength but carry a slightly higher risk of rupture and
- Self-expanding valves, which can conform better to an elliptical annulus but may have higher rates of paravalvular leakage.
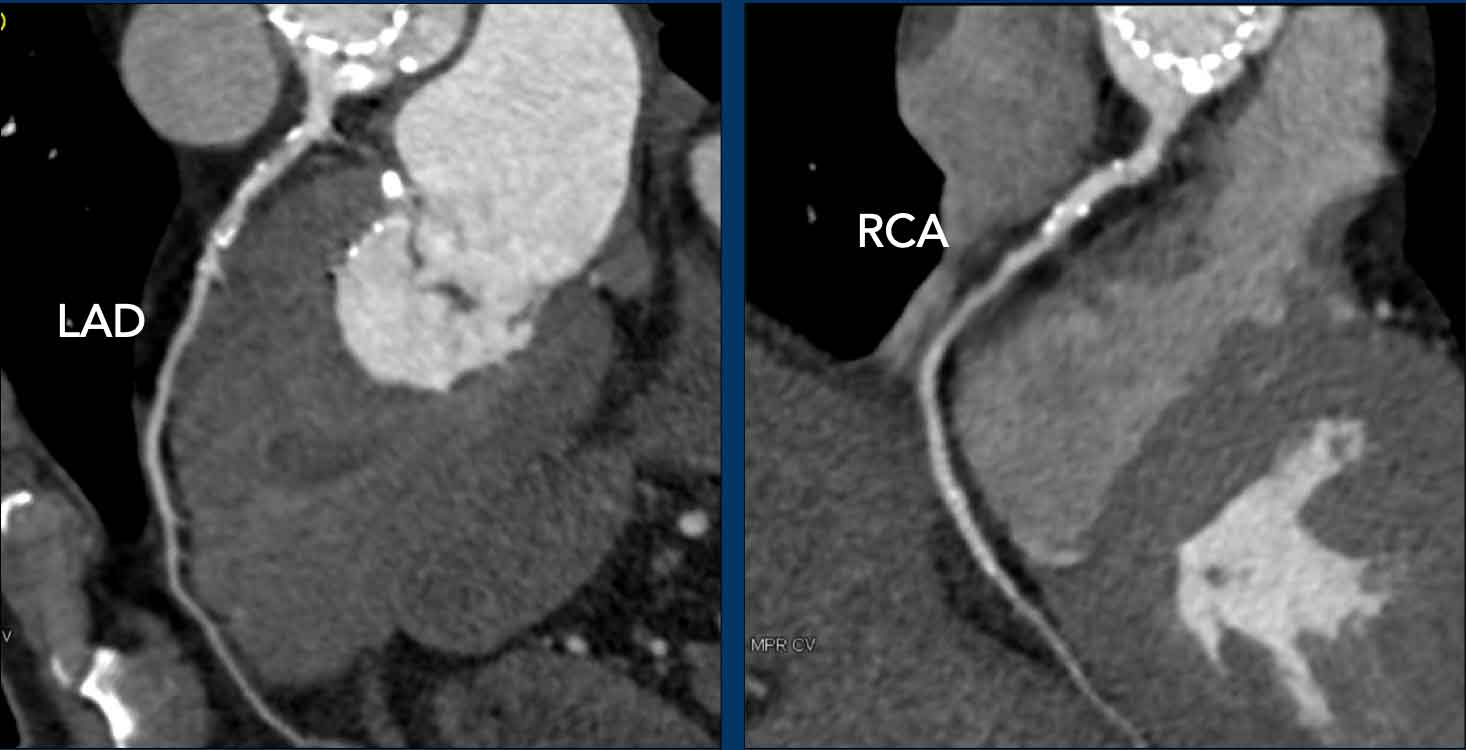
Coronary assessment
Historically, every patient preparing for
a TAVI underwent an invasive coronary angiography (ICA) to exclude significant
coronary artery disease (CAD).
Today, CTA can be used to exclude severe CAD
before TAVI though the rate of patients with severe calcium and non-diagnostic
scans will be higher compared to a dedicated cardiac CTA.
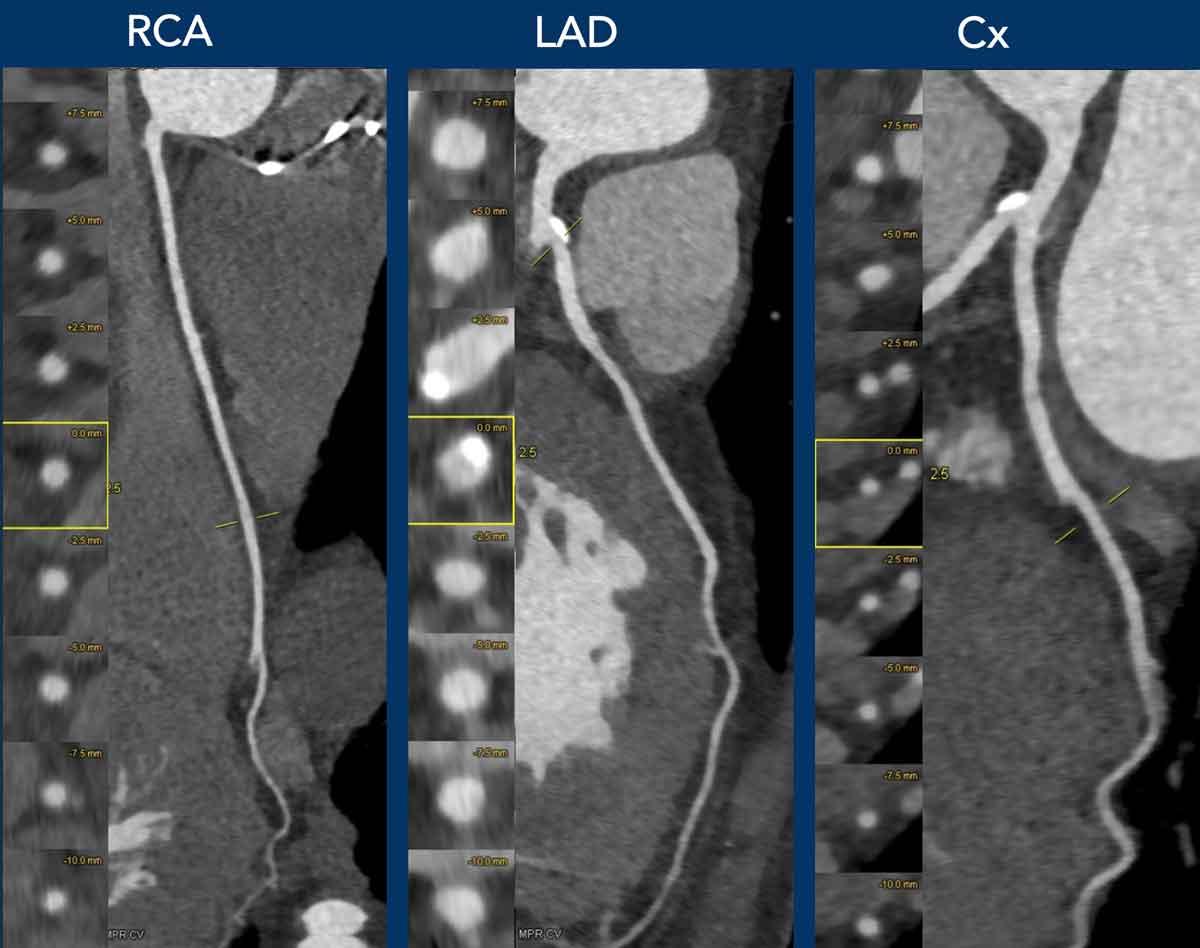
Images
75-year-old female, no
nitroglycerin or beta-blockers were administered.
Significant coronary artery
disease was excluded.
Vascular Access
CT provides a comprehensive evaluation of the vascular system, allowing assessment of vessel tortuosity, stents, dissections, calcification and diameter.
A critical metric derived from CT is the minimal luminal diameter. However,
luminal diameter must be cross-referenced with the distribution of
calcification.
Most contemporary TAVI delivery systems require a minimum common femoral
artery diameter of 5.0
to 5.5 mm to
safely accommodate the sheath (typically 14F to 16F) without causing vascular
injury.
Finally, TAVI requires dual access.
While the primary large-bore site delivers the valve, a secondary,
smaller-bore access (often contralateral femoral or radial artery) accommodates
a pigtail catheter for angiographic visualization during deployment.
Video
Overview of vascular access.
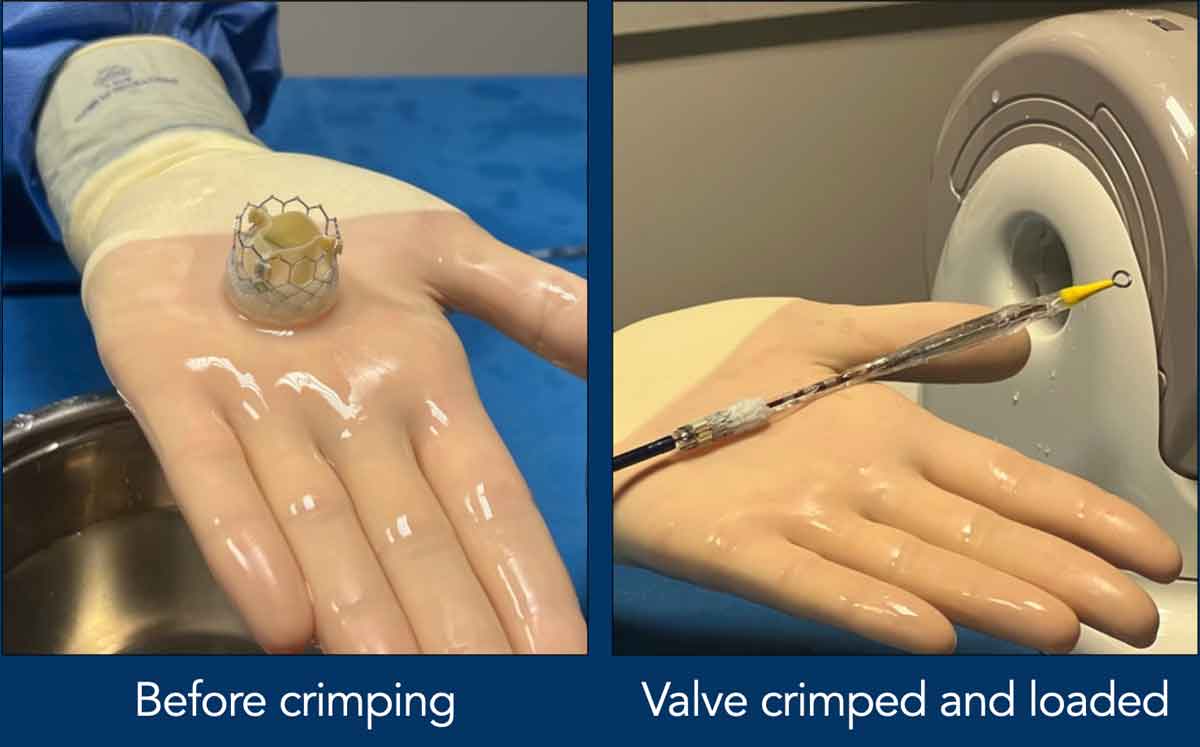
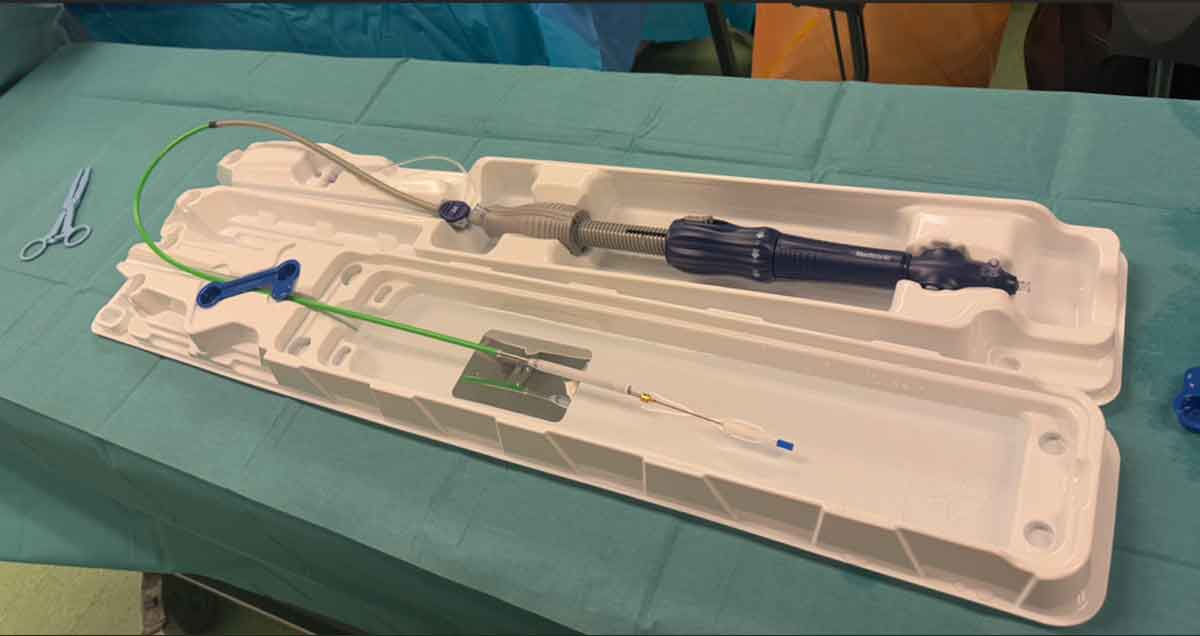
Images
Balloon expandable valve loaded on a catheter.
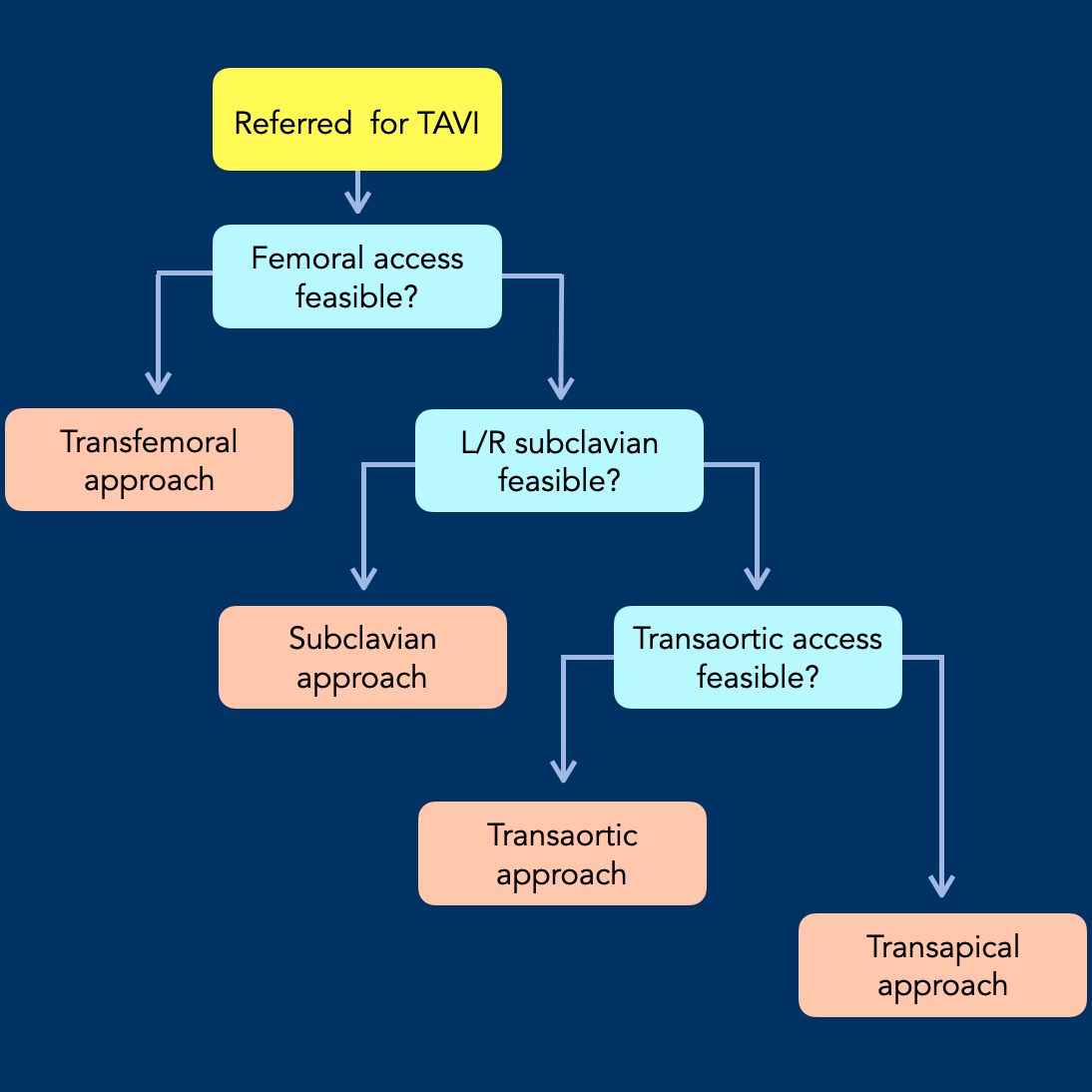
Access route
While transfemoral access remains the preferred route for TAVI, a subset of patients presents with distinct vascular anatomy (e.g., extreme tortuosity) or severe peripheral artery disease, that precludes a transfemoral access.
Alternative access routes are:
- Subclavian approach
- Preferably the left subclavian artery due to its favorable anatomical angle and shorter distance to the aortic annulus.
- Transaortic access
- Involves a mini-sternotomy or a right parasternal incision to directly expose the ascending aorta.
- A purse-string suture is placed on the anterior wall of the aorta, and a sheath is inserted directly into the ascending aorta.
- The transcatheter valve is then advanced across the aortic valve.
- Transapical access (fewer than 0.5% of cases)
- The procedure involves a mini-thoracotomy to expose the apex of the heart.
- A purse-string suture is placed at the apex, and a sheath is inserted directly into the left ventricle.
- The transcatheter valve is then advanced across the aortic valve.
Flowchart adapted from (4).
This illustration displays an algorithm for determining the appropriate access route for
TAVI.
The selection process is sequential, prioritizing the least invasive
method.
Complications of TAVI
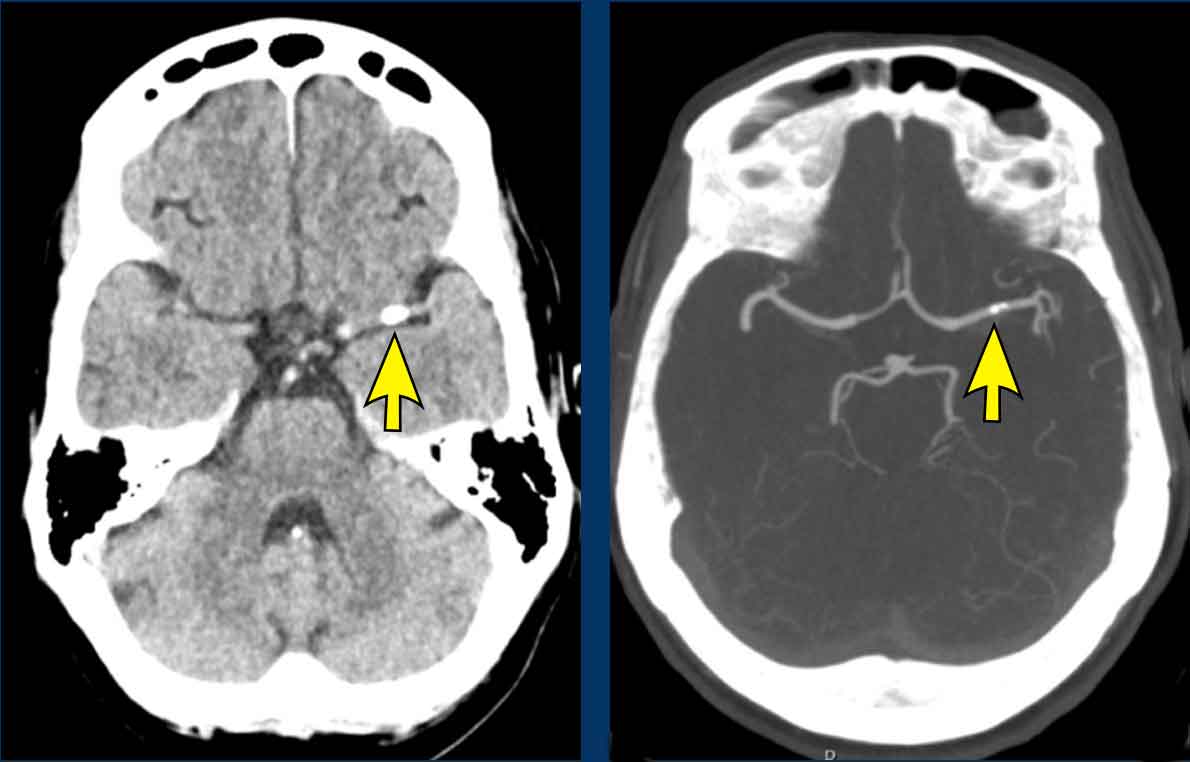 Calcified thrombus in left M1 (arrow). Minutes after TAVI procedure dysarthria and weakness of the right arm and right leg were observed. Patient recovered without intervention.
Calcified thrombus in left M1 (arrow). Minutes after TAVI procedure dysarthria and weakness of the right arm and right leg were observed. Patient recovered without intervention.
Stroke
TAVI is increasingly performed due to its expanded indications for younger, lower-risk patient populations.
For radiologists, recognizing six major complications is critical. (5).
Strokes following TAVI are classified into two categories based on timing:
- Acute/Early Strokes
- Timing: Occur within 24 to 72 hours post-procedure.
- Incidence: Account for ~50% of all TAVI-related strokes.
- Mechanism: Almost always embolic and procedure-related.
- During the TAVI procedure mechanical forces can dislodge pieces of calcium, cholesterol, or valve tissue, which can embolize into the brain.
- Late Strokes
- Timing: Occur weeks to months after the procedure.
- Rarely related to procedural debris
- Typically driven by patient-specific factors, most commonly atrial fibrillation.
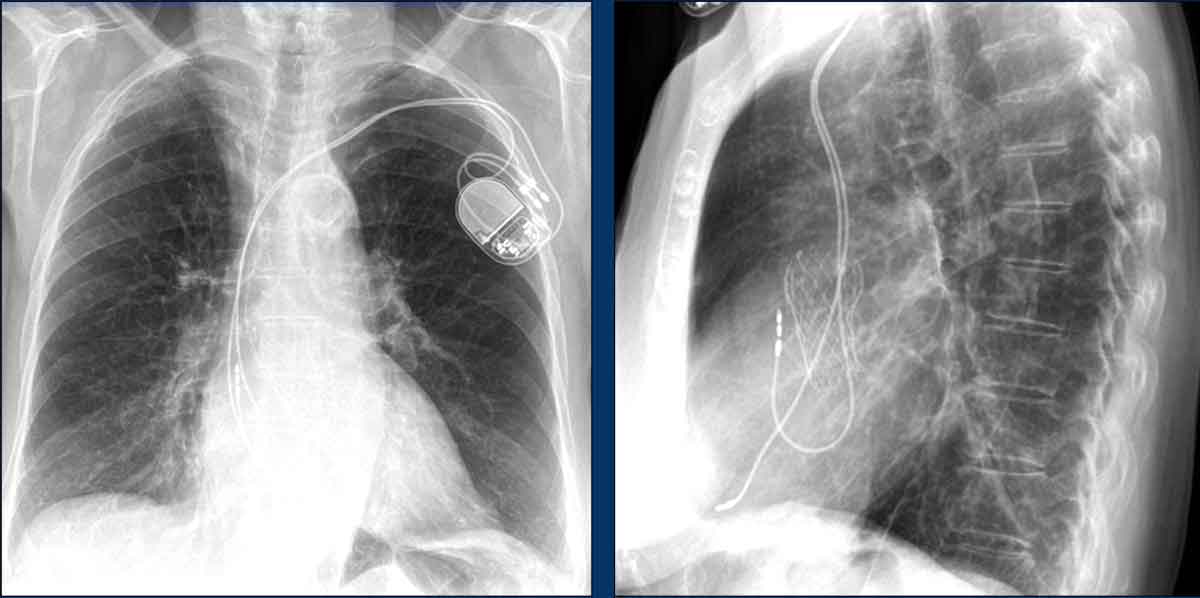
AV block
One of the most common complications of TAVI is mechanical injury to the cardiac conduction system, frequently necessitating permanent pacemaker (PPM) implantation—typically during the index hospitalization.
The risk is significantly elevated in patients with a pre-existing right bundle branch block.
Image
Post-TAVI pacemaker with leads in the right atrium and right
ventricle.
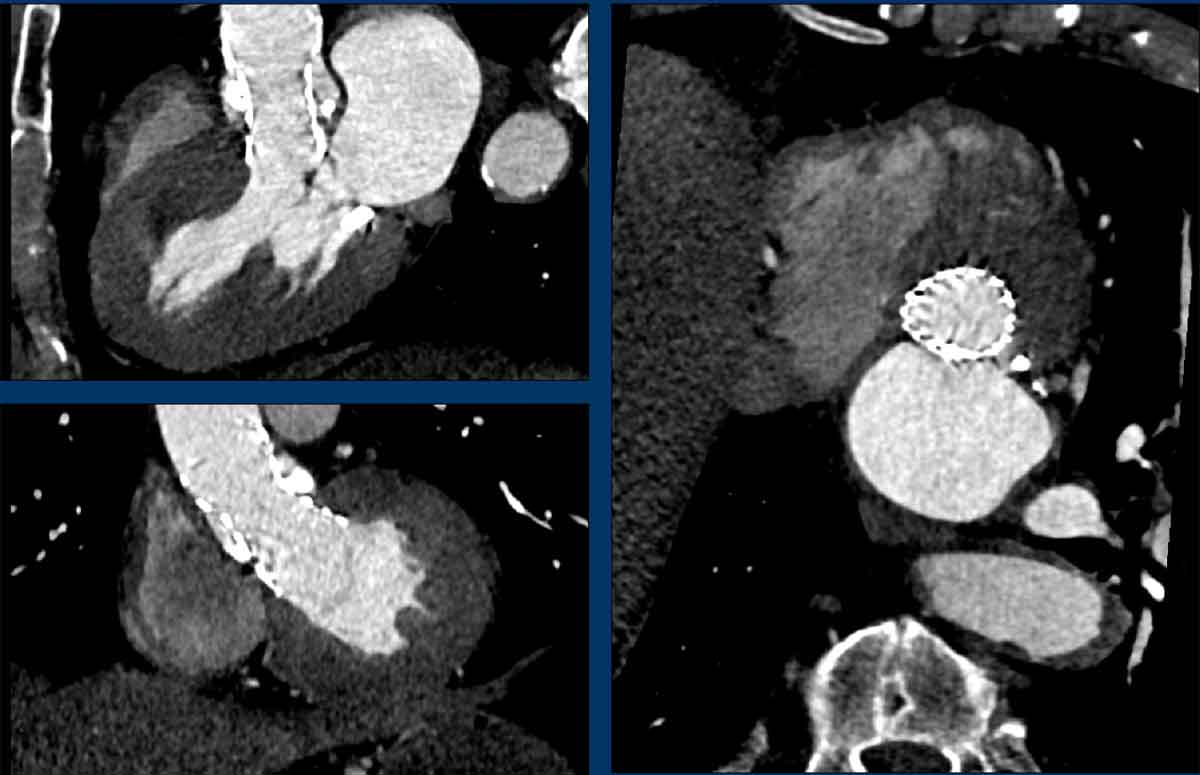
Paravalvular leakage
The TAVI valve is implanted directly within the native, calcified aortic valve.
If calcific deposits prevent the new metallic frame from achieving a complete, flush seal against the aortic annulus, paravalvular regurgitation may occur during diastole.
Thanks to precise valve sizing and the incorporation of outer sealing skirts, severe paravalvular leak occurs in less than 1% of cases with balloon-expandable valves.
The presence of paravalvular leakage is assessed intraprocedurally following valve deployment using transthoracic echocardiography (TTE).
If needed, cardiac CT angiography (CTA) can also be utilized.
Symptomatic leakage may be managed with post-dilatation of the bioprosthesisor the use of paravalvular closure devices.
Images
Post
TAVI CTA. No paravalvular leakage was detected
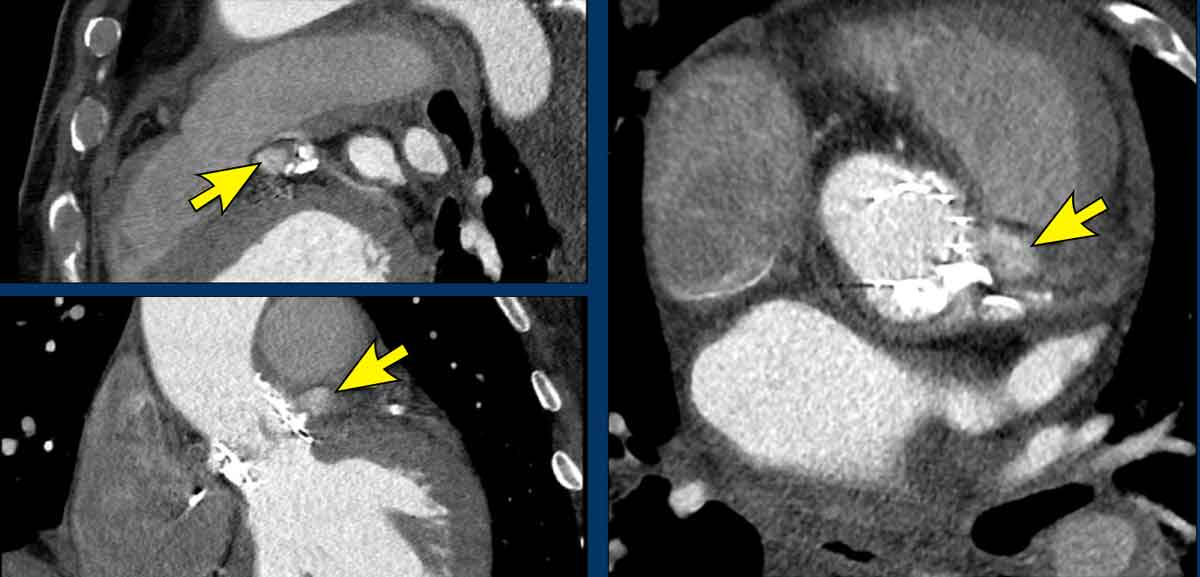 Contained rupture at left coronary cusp.
Contained rupture at left coronary cusp.
Annular rupture
TAVI carries a rare but potentially catastrophic risk of aortic root or
annular rupture, typically occurring during valve deployment.
Risk factors include extensive LVOT calcification and valve oversizing.
To reduce this risk, higher valve implantation is recommended in the
presence of severe LVOT calcification.
Management depends entirely on the severity of the tear. A contained rupture allows for a conservative approach, often managed with close observation and pericardiocentesis - whereas an uncontained rupture triggers rapid cardiac tamponade and cardiogenic shock, requiring emergent open-heart surgery.
 Coronary obstruction was suspected. None was seen on post TAVI CT.
Coronary obstruction was suspected. None was seen on post TAVI CT.
Coronary obstruction
Coronary artery obstruction is a rare (under 1%) but serious
complication of TAVI, carrying a high mortality rate that is closely linked to
the failure of coronary revascularization (7).
It typically occurs when the bulky, calcified native aortic leaflets are
pushed outward by the expanding valve prothesis, effectively sealing the
coronary ostia and cutting off blood supply to the heart muscle.
Anticipating this risk through CT scanning allows for preventive
intraprocedural measures.
Key Risk Factors
- Low coronary height: Ostia located less than 10-12 mm from the aortic annulus.
- Narrow sinuses of Valsalva: Leaving inadequate space to accommodate the displaced native leaflets.
- Valve-in-valve procedures: Teating a degenerated bioprosthesis carries a significantly higher risk of coronary obstruction.
Vascular complications
Vascular complications remain a significant source of morbidity in TAVI
and are primarily driven bt the relative large sheath size (figure).
While major bleeding typically originates from the access site, other critical
bleeding locations - most notably the pericardial
space leading to effusion or tamponade – can also occur.
A failed percutaneous closure demands immediate interventional bailout strategies, such as prolonged balloon tamponade or covered stent implantation, to control acute hemorrhage.
Delayed vascular complications include pseudoaneurysms, which develop when an arterial puncture fails to seal, creating a pulsating, blood-filled sac adjacent to the vessel.
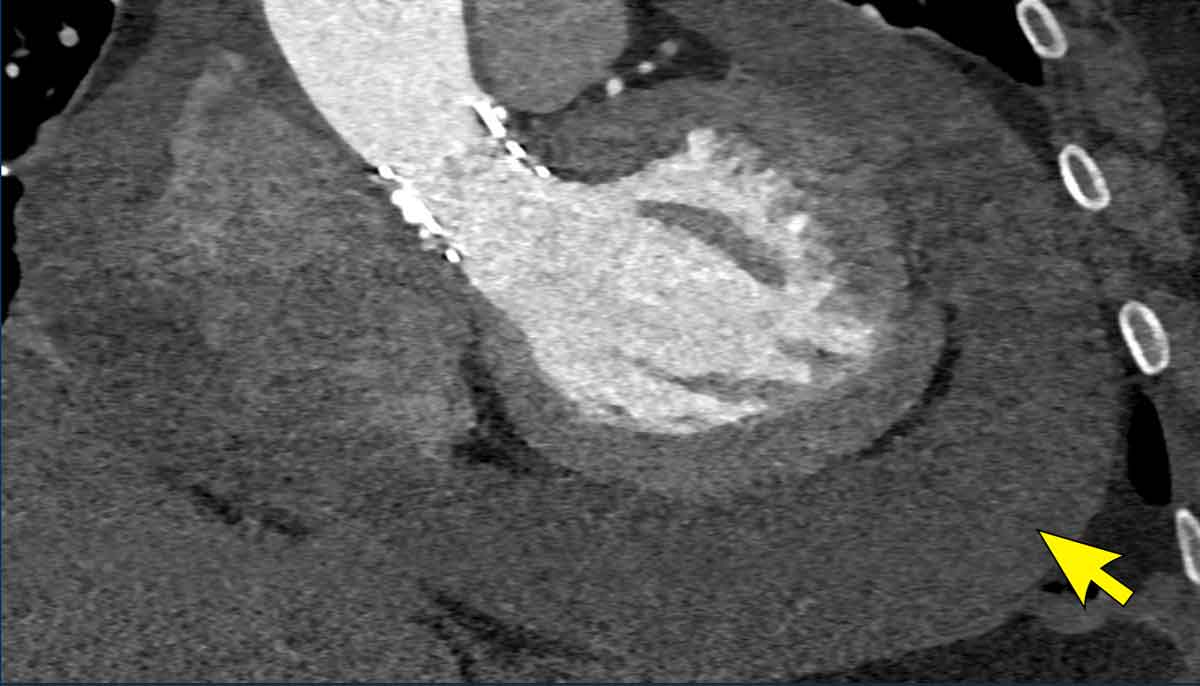
Pericardial Bleeding
Pericardial bleeding - including pericardial effusion, tamponade, or annular rupture - is observed in ~1–5% of TAVI cases. It represents a hyper-acute, life-threatening complication.
The etiologies of post-TAVI pericardial hemorrhage include:
- Annular or aortic root rupture: Due to oversizing of the valve, forceful balloon post-dilation, or calcification-related fragility of the LVOT/aortic root.
- Myocardial perforation by guidewires, catheters, or delivery systems. Especially in tortuous or heavily calcified anatomies.
- Transapical access complications: Direct myocardial or pericardial injury during apical puncture.
Image
Pericardial bleeding after
TAVI, confirmed during pericardiocentesis.
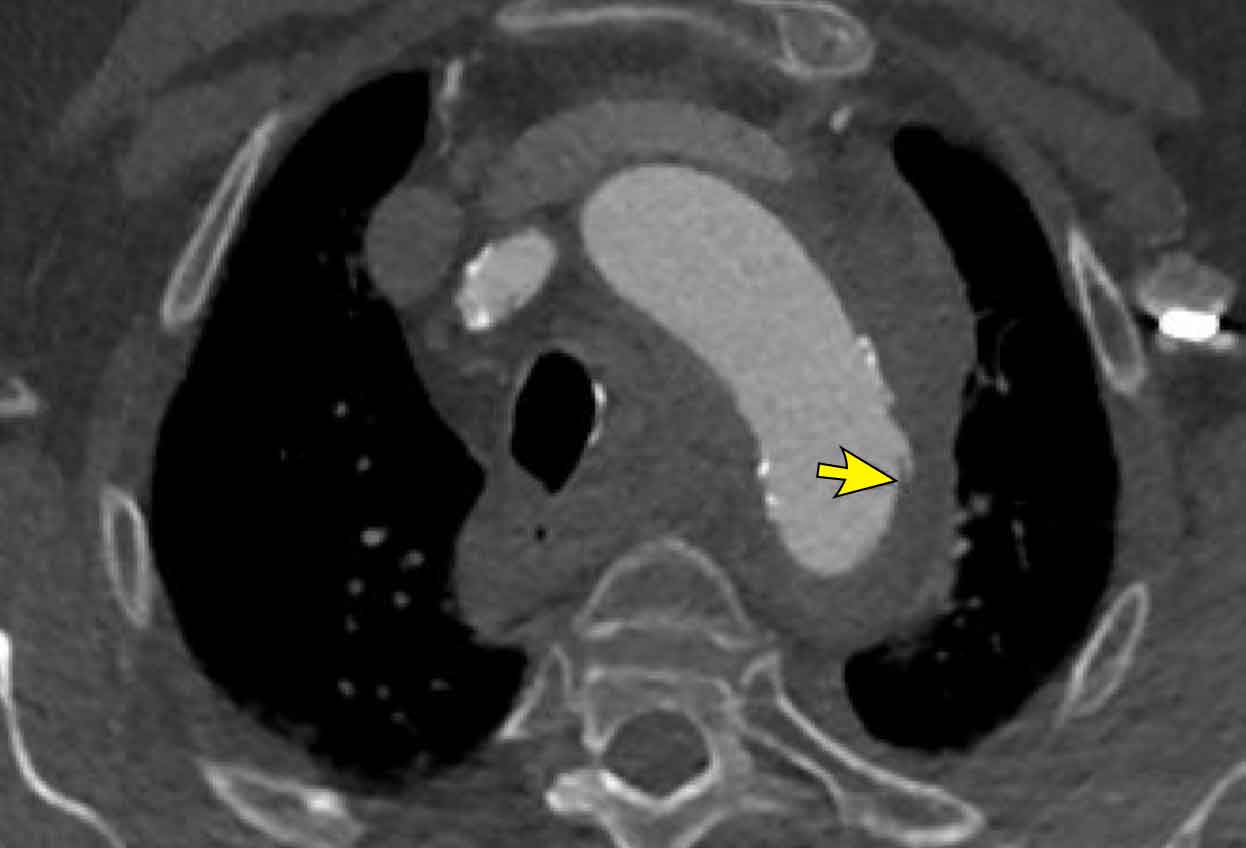
Aortic dissection
Aortic dissection TAVI is an exceptionally
rare complication.
Arterial dissection usually occurs during sheath insertion
in vessels with severe tortuosity or heavy calcification.
Image
Subtle intima flap (arrow) and
intramural hematoma in the aortic arch.
Pseudo-aneurysm
Play movie
Due to heavy calcification at the level of the femoral artery, a high access puncture was chosen.
A post-procedural pseudoaneurysm with bleeding developed. which was treated with a covered stent (8x40 Covera).
Play movie
The pseudo-aneurysm which treated with a covered stent (8x40 Covera).
Potential valve complications
HALT and HAM
Hypoattenuated leaflet thickening (HALT) and hypoattenuation affecting motion (HAM) can be observed on cardiac CT scans after TAVI.
HALT refers to a thrombus forming on the new bioprosthetic valve's
leaflets.
When this clot thickens enough to physically restrict the leaflets from opening
and closing properly - a phenomenom also describes as reduced leaflet motion
(RELM) -, it progresses to HAM (8).
Subclinical leaflet thrombosis is highly dynamic
over time, frequently appearing within the first few months post-procedure.
Video
CTA demonstrating HALT and
HAM of the neo right coronary cusp.
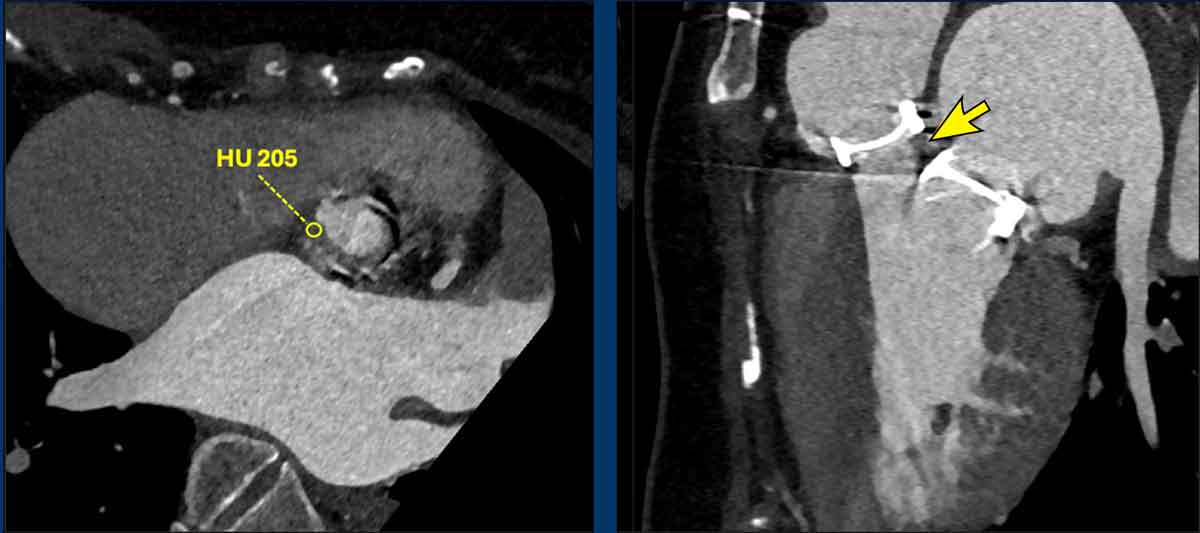
Pannus
Pannus refers to the
overgrowth of dense, fibrous scar tissue that typically originates at the valve
annulus and propagates along the base of the leaflets.
Images
Subvalvular pannus with high attenuation (arrow)
Vegetation
This refers to an infectious mass that can attach unpredictably anywhere on the leaflets, annulus, or stent frame.
Timely identification of these complications may require additional measures such as antithrombotic treatment, valve-in-valve treatment or surgical valve replacement.
Video
Vegetation on the right coronary cusp. Vegetation and aortic
valve removed during surgery.
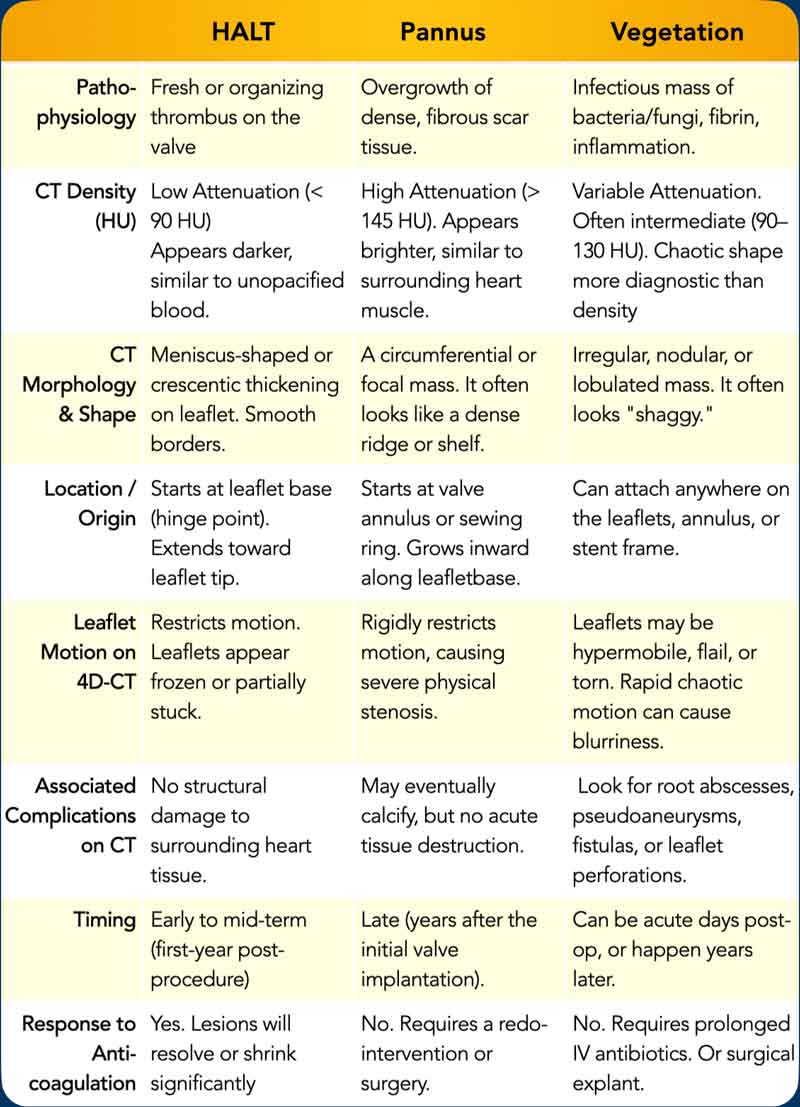
Overview of the features of HALT, Pannus and Vegetation
Reference
for HU value (9,10).