Lung Adenocarcinoma
The chameleon in lung oncology
Onno Mets¹, Emile Comans² and Robin Smithuis³
¹Amsterdam UMC, ²Haaglanden Medical Center, the Hague, and ³Alrijne Hospital, Leiden, the Netherlands
Publicationdate
Lung adenocarcinoma is the most common histological subtype of lung cancer encountered in clinical practice. It demonstrates a broad spectrum of morphological and radiological manifestations, resulting in greater heterogeneity than other primary lung malignancies, such as squamous cell carcinoma and small cell lung carcinoma.
On imaging, lung adenocarcinoma may mimic a variety of benign pulmonary conditions, including:
- Pneumonia
- Focal ground-glass opacity
- Simple pulmonary cyst
Familiarity with these imaging patterns, together with an understanding of the underlying histopathological correlates, is essential for accurate recognition and early diagnosis of these tumors.
This article provides an overview of the diverse imaging appearances of lung adenocarcinoma, emphasizing its potential to be misinterpreted and the consequent risk of delayed diagnosis.
We thank pathologist Rieneke Britstra for her contribution and comments on the histopathology presented in this article.
Lung Cancer Types
 Small cell lung cancer
Small cell lung cancer
Small cell lung cancer
Lung cancer can be categorized into small cell lung cancer (SCLC) and non-small cell lung cancer (NSCLC). The majority (~85%) of lung cancers are NSCLC, with adenocarcinoma accounting for over 50% of these cases, making it the most common type encountered in clinical practice.
In contrast to adenocarcinoma, SCLC and squamous cell carcinoma (SqCC) typically present as more characteristic malignant lesions, often exhibiting a consistent morphology of solid, irregular, or spiculated nodules or masses. Both types are strongly associated with a history of smoking.
Small cell lung cancer generally appears as:
- Relatively small solid nodule (arrow)
- Accompanied by disproportionately large lymphadenopathy
- Frequently, metastatic disease at the time of diagnosis.
While FDG-PET is not
routinely used in the initial workup as per clinical
guidelines, it will invariably show high metabolic activity.
Example
A small solid lesion in the basal
right upper lobe (arrow), and bulky heterogeneous/necrotic lymphadenopathy in de hilum
and mediastinum.
FDG-PET CT shows intense metabolic activity.
 Squamous cell carcinoma. No lymphadenopathy.
Squamous cell carcinoma. No lymphadenopathy.
Squamous cell carcinoma
Squamous cell carcinoma typically manifests as
- Solid lesion, not infrequently with central necrosis or cavitation.
- Tends to have a more central location as it originates from the bronchial squamous epithelium and may cause obstruction with post-obstructive changes (arrow).
- Lymphadenopathy is less common in the early stages, and the nodes present in such cases are usually reactive to the obstruction and may show enhancement in contrast-enhanced CT.
- FDG-PET always shows marked metabolic activity of the primary lesion, even in small lesions (see figure).
Example
Irregular solid mass in the right
lower lobe.
Oclusion of a subsegmental bronchus (arrow).
No post-obstructive
changes.
Intense FDG uptake in the lesion.
Absence
of lymphogenic metastases.
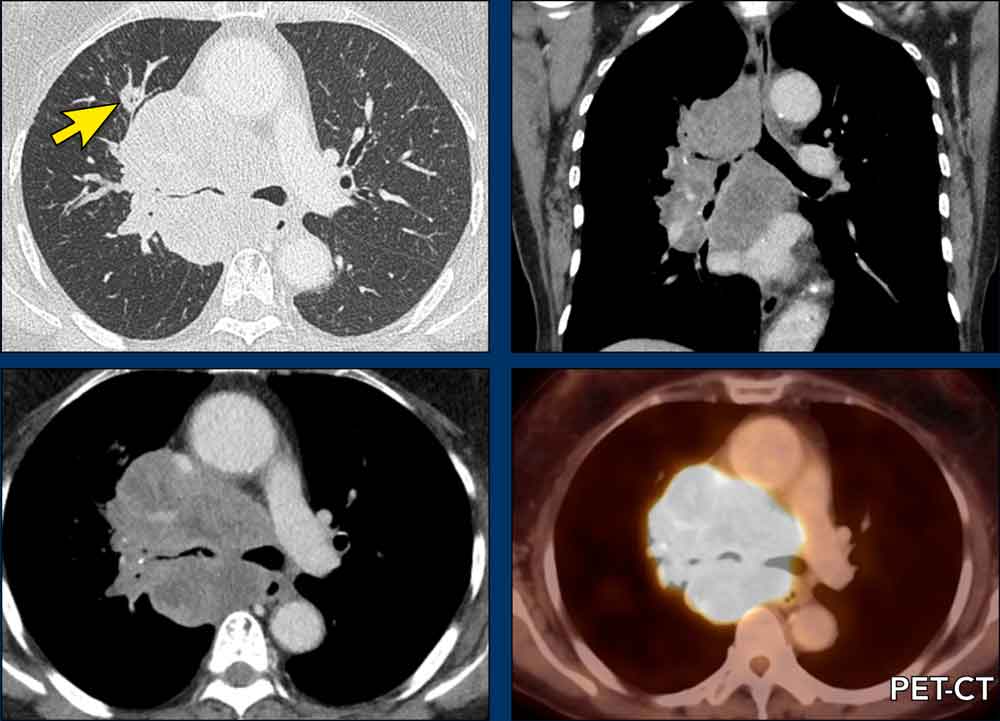
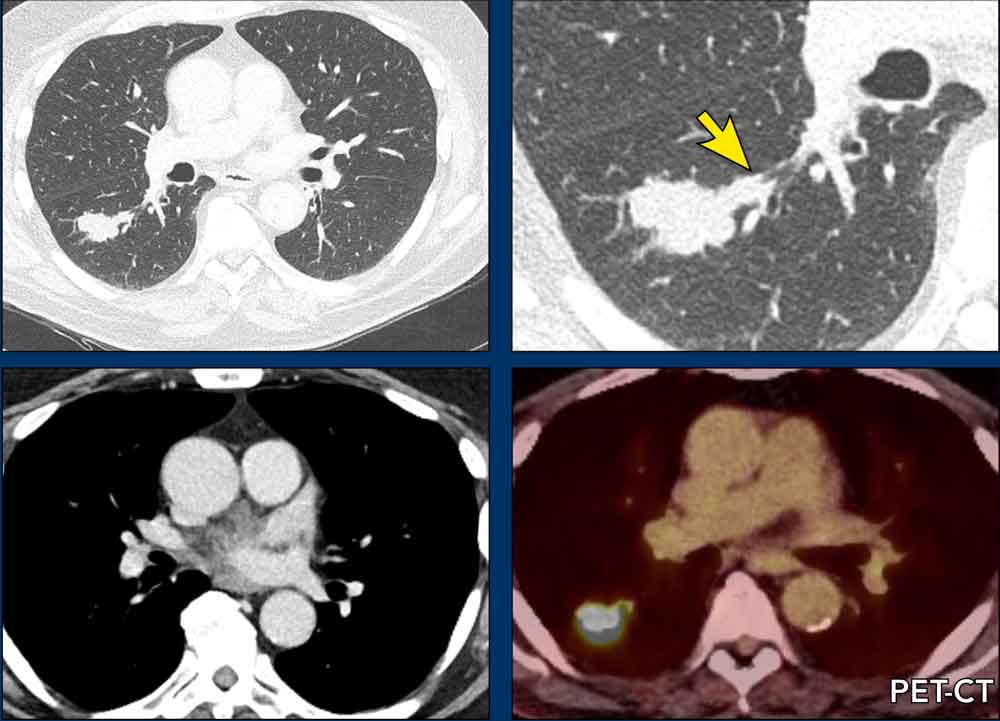
Adenocarcinoma
This lung tumor exhibits significant heterogeneity in both imaging characteristics and metabolic behavior.
Its radiographic appearance can vary widely and present as:
- Slow-growing subsolid nodules
- Aggressive solid masses
- Lobar consolidation
FDG-PET activity in adenocarcinoma may range from markedly elevated to nearly absent, which complicates imaging interpretation and can potentially delay accurate diagnosis.
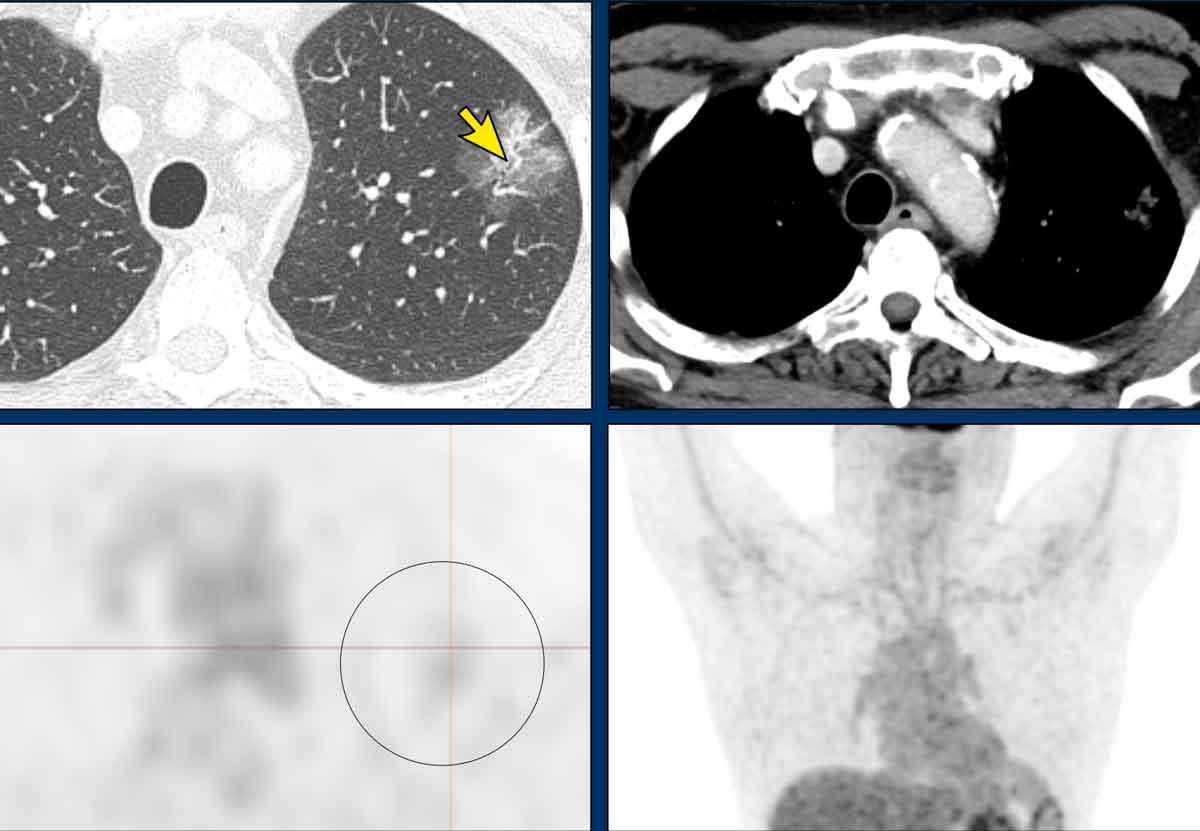
Examples
Four different presentations of adenocarcinoma of the lung.
Notice subsolid presentation (arrow).
Histopathological Growth Patterns
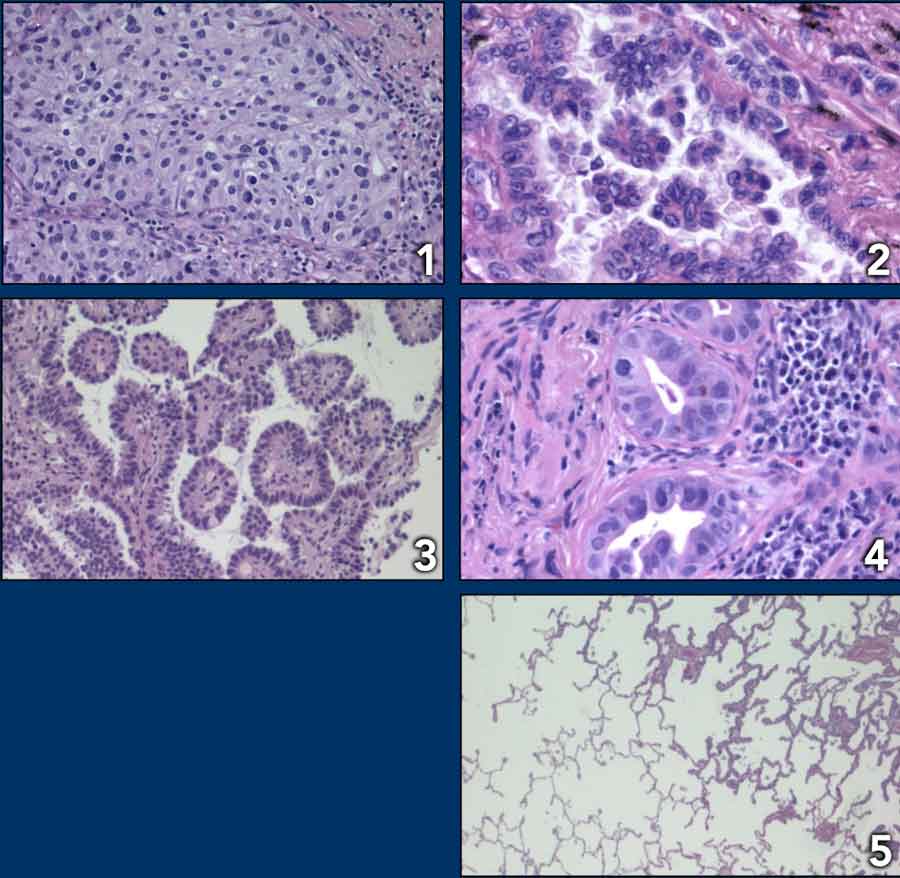
Lung adenocarcinoma exhibits several distinct histopathological growth patterns, each contributing to variations in imaging appearance.
Pathologists classify growth patterns in:
- Solid adenocarcinoma
Characterized by polygonal tumor cells arranged in sheets, with no identifiable lepidic, acinar, papillary, or micropapillary architecture. - Micropapillary adenocarcinoma
Defined by tumor cells forming papillary tufts (florets) without fibrovascular cores, which may be attached to or detached from alveolar walls. - Papillary adenocarcinoma
Features glandular tumor cells growing along the surface of fibrovascular cores. - Acinar adenocarcinoma
Exhibits glandular structures with central luminal spaces surrounded by tumor cells. - Lepidic adenocarcinoma
Composed of bland pneumocytic cells (type II pneumocytes or club cells) growing along alveolar walls.
Prognosis generally improves from top to bottom on this list.
It is common for multiple patterns to coexist within a single tumor, with a pattern being acknowledged if it comprises more than 5% of the tumor volume.
Tumors are classified into subtype according to the predominant architectural pattern. This is why you may encounter descriptions like "acinar predominant (~60%) adenocarcinoma of the lung, with large lepidic components (~40%)."
Lepidic growth
Lepidic growth is a surface-spreading pattern where tumor cells grow along intact alveolar walls, preserving lung architecture and aeration. On CT, these lesions appear as ground-glass opacities.
- Pure lepidic growth (≤30 mm): Classified as adenocarcinoma in situ (AIS, Tis).
- Lepidic growth (>30 mm): Classified as lepidic-predominant adenocarcinoma, even if morphologically AIS.
If airspaces are filled by tumor cells or focal atelectasis, CT shows a part-solid appearance. Histopathology is required to distinguish minimal invasion from atelectasis.
Metabolic activity on FDG-PET
FDG uptake happens in:
- Cells that are low in oxygen or
- Cells that break down glucose into lactate even in the presence of oxygen (called aerobic glycolysis), which is frequently seen in cancer cells.
FDG
uptake in relation to growth pattern
Even if
the tumor cells have a preference for aerobic glycolysis, FDG uptake in pure or
predominant lepidic (ground glass) lesions is typically minimal. This is explained by the
limited tumor cell mass in this surface-spreading growth pattern, along with
the aerated alveolar spaces.
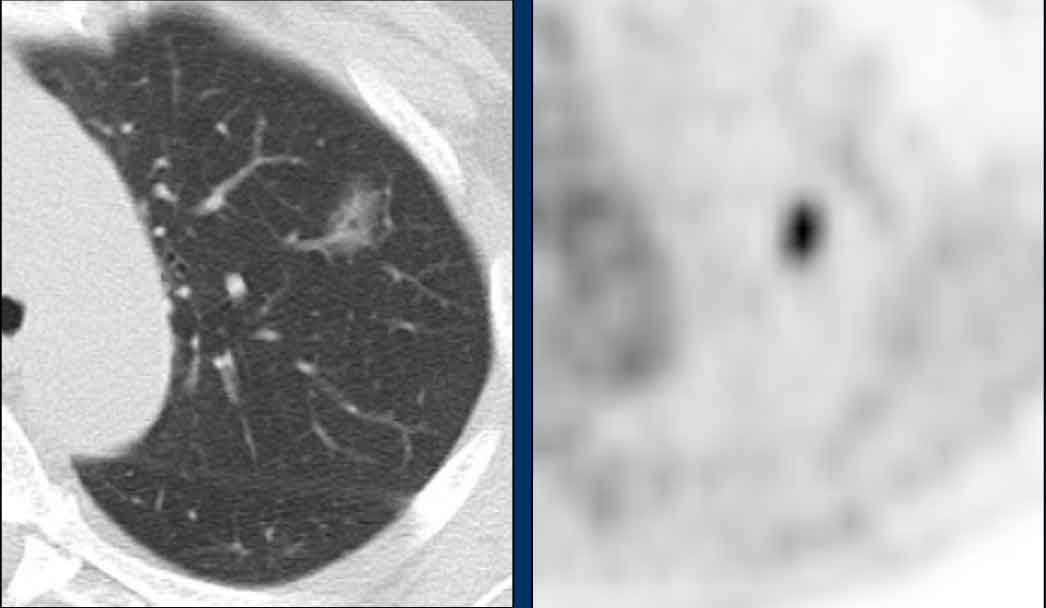
Images
- Pure ground-glass lesion in the left upper lobe with faint FDG uptake (circle)
- Part-solid lesion in the right lower lobe. The solid component shows focal intense FDG uptake, likely corresponding to the invasive portion.
- Both findings are consistent with lesions within the adenocarcinomatous spectrum.
If a ground glass lesion demonstrates intense FDG uptake, infection should be strongly favored over malignancy.
Images
- Ground glass lesion in the left upper lobe
- Intense FDG-uptake
This proved to be infection
For
other types of adenocarcinoma, FDG uptake will generally be focussed in the
more solid, presumably invasive component.
Nevertheless, it may vary from
minimal to intense.
This parameter is thus of limited value in lung
adenocarcinomas, and should therefore be used very cautiously in distinguishing
benign from malignant.
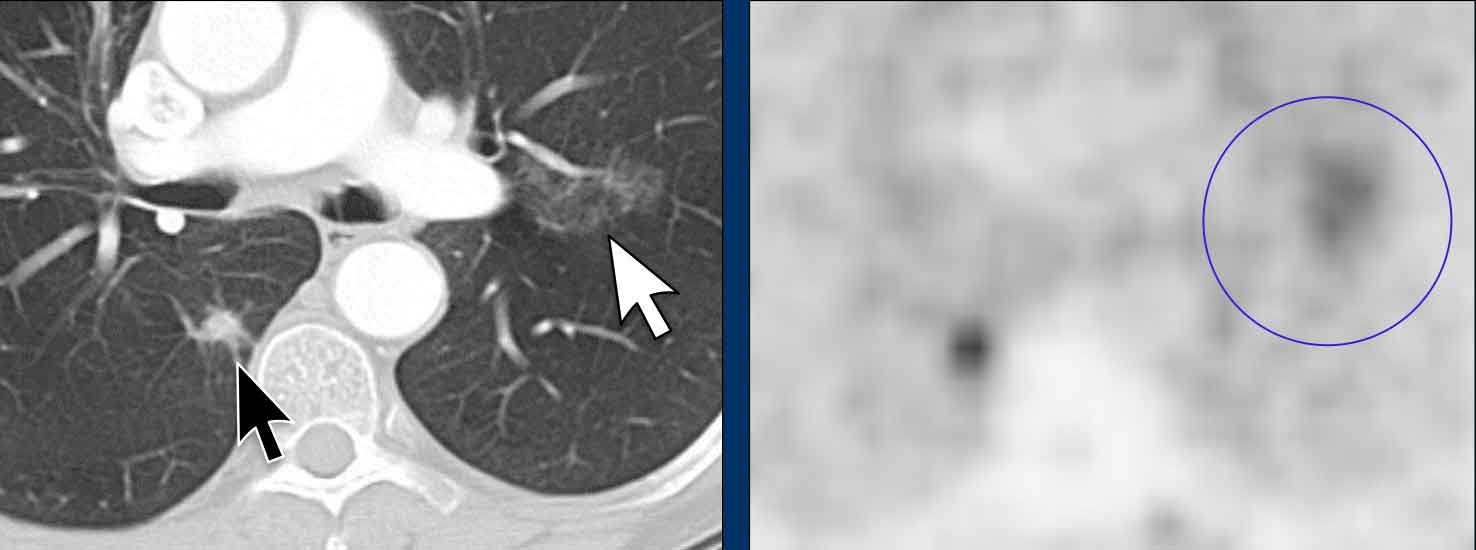
Images
- Large subsolid lesion with mainly ground glass component.
- Subtle intralesional bronchiectases (arrow).
- Minimal traction on the pleura.
- This represents a morphologically highly suspicious lesion, especially when persistence has been shown over time.
Histopathology
40 mm lepidic predominant adenocarcinoma with limited invasive growth.
The PET scan shows only mild FDG
uptake in the more solid component and otherwise limited signal, which is
consistent with the above.
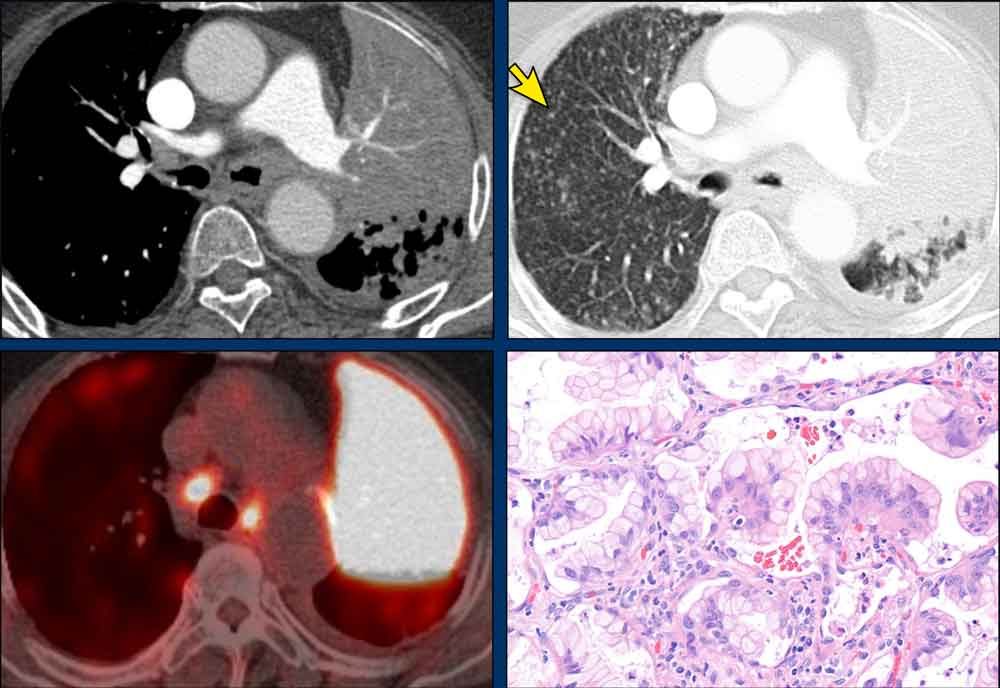
Pitfalls in metabolic activity
Extracellular mucin (or rarely necrosis) in adenocarcinoma can reduce FDG uptake, as these areas lack viable tumor cells.
Thus, mucinous adenocarcinomas may appear as hypodense, heterogeneous lesions with low metabolic activityon imaging—yet they remain primary lung malignancies.
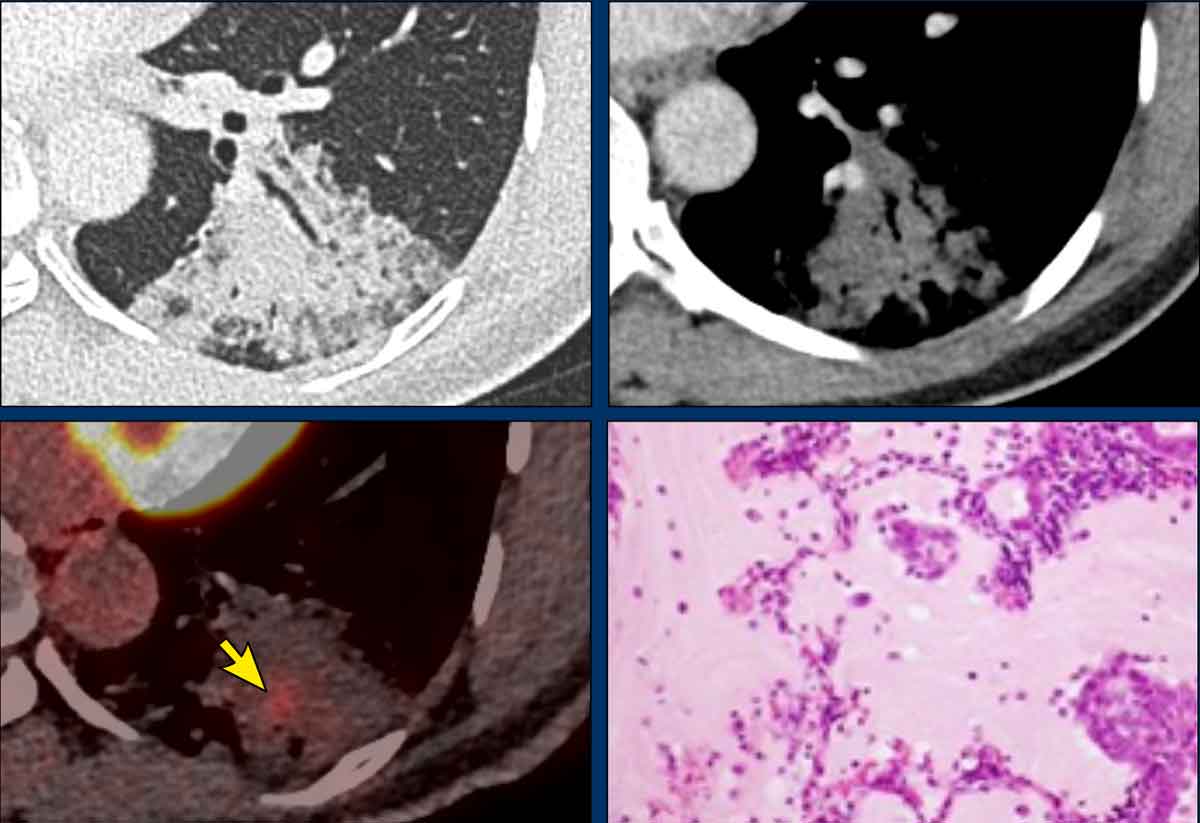
Images
In
the left lower lobe, a persistent consolidative lesion despite treatment with
antibiotics and steroids, after initial suspicion for pneumonia.
FDG uptake was low and heterogeneous.
This should not be mistaken for evidence
of benign disease.
Pathology
Mucinous adenocarcinoma of the lung with partially lepidic growth.
Low FDG uptake due to the extensive mucinous lakes (pale pink areas without viable tumor cells),
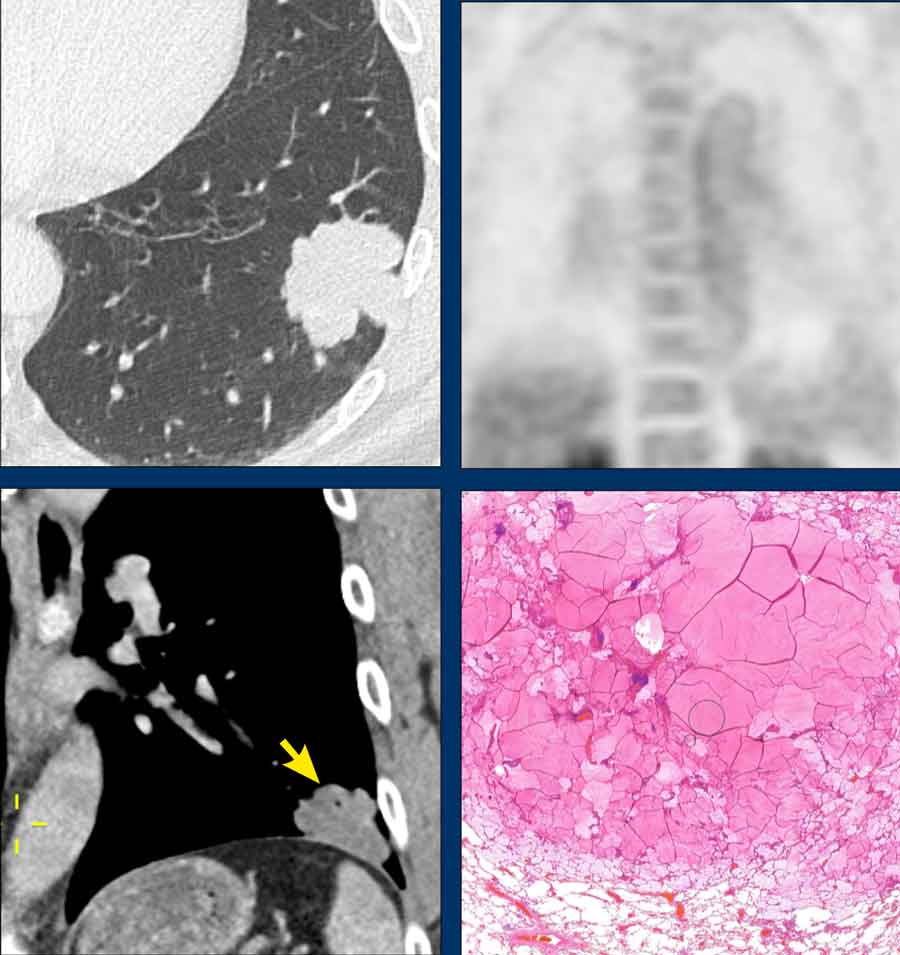
Absence of FDG uptake in adenocarcinoma
Colloid adenocarcinoma is a subtype of mucinous lung adenocarcinoma defined by abundant
extracellular mucin that fills and expands the alveolar spaces, leading to
destruction of the surrounding lung parenchyma.
Owing to this high mucin
content, lesions typically appear hypodense on imaging and may show little to
no FDG uptake on PET scans, despite their malignant nature.
Images
- Hypodense solid mass in the left lower lobe (arrow) characteristic of colloid adenocarcinoma.
- The minimal number of tumor cells present in between the mucin (as seen on the magnification view) may pose both imaging and pathological challenges in accurately diagnosing this relatively indolent malignancy.
Pneumonic type of Lung Adenocarcinoma
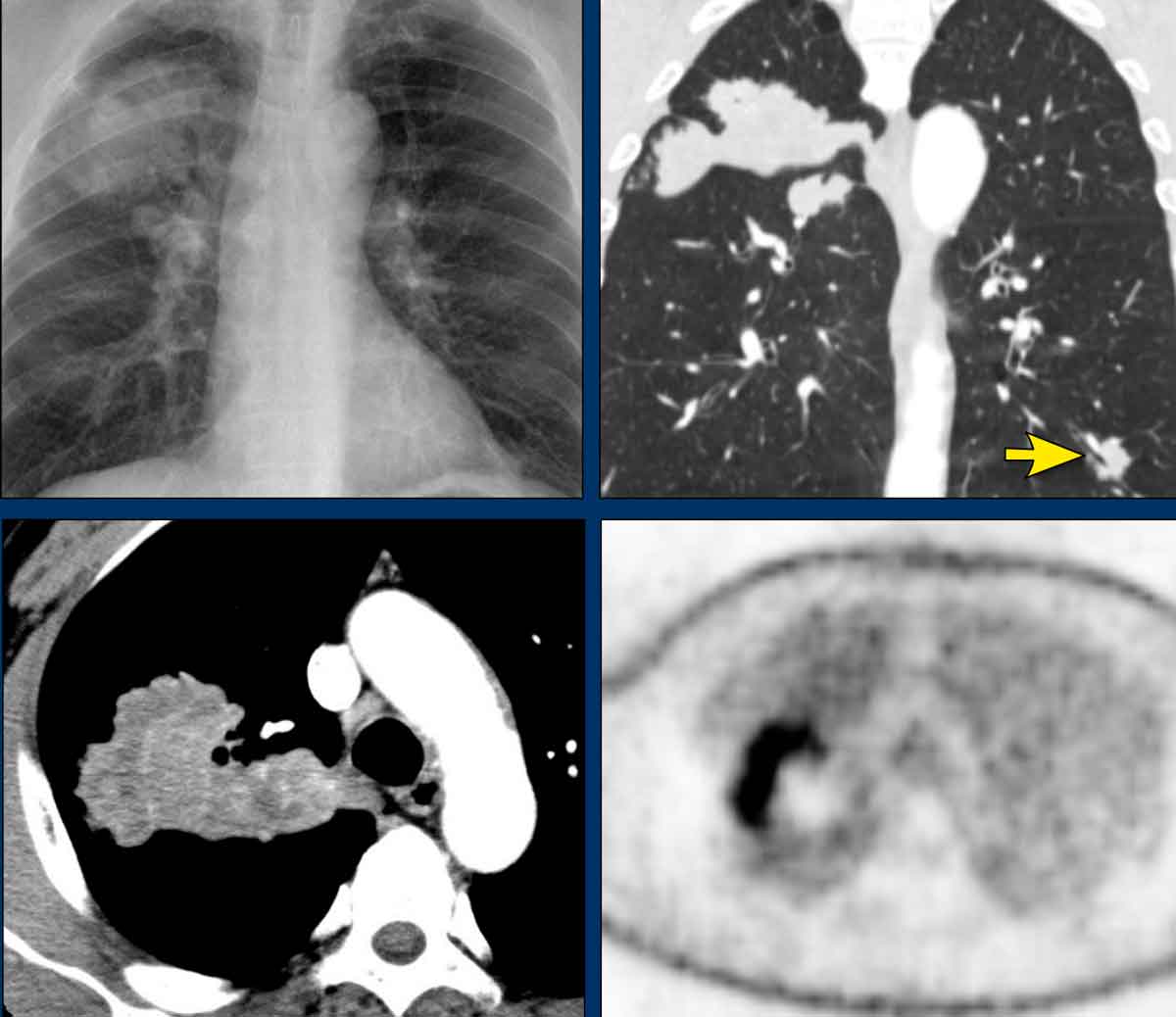
Pneumonic type of Lung Adenocarcinoma (PLADC) is a
form of invasive often mucinous adenocarcinoma typically characterized by
heterogeneous, hypodense consolidative appearance.
The hypodensities are caused
by the mucinous components.
It often presents as a larger, consolidative lesion
with multicentric disease, surrounding ground-glass and sometimes separate
nodular components due to alveolar tumor spread (Spread-through-airspaces (STAS).
Its tendency for spread through airspaces contributes to the risk of pulmonary recurrence and aerogenic metastases, while lymphatic spread and distant metastatic disease are less common.
Images
- Chest X-ray: consolidation detected after presentation with persistent cough and dyspnea, but only mild lab abnormalities and no fever.
- CT: multicentric consolidation with
heterogenous hypodense appearance typical for PLADC.
Notice node in left lower lobe (arrow) - FDG-PET: only partial metabolic activity in the right upper lobe on due to mucinous components.
PLADC is often misdiagnosed or diagnosed late, particularly in nonsmokers.
It can mimic pneumonia, presenting with consolidations, dyspnea, cough, and occasionally fever.
Due to its infectious-like appearance, it is frequently initially treated as pneumonia and only identified later when symptoms persist.
Early recognition depends on clinical awareness and a high index of suspicion.
A mismatch between clinical findings and the apparent severity of infection should raise consideration of PLADC.
Images
- Hypodense lobar consolidation in the left upper lobe, with comparable changes in the apex of the left lower lobe
- Bilateral small nodular opacities (arrow).
Further work-up showed invasive mucinous adenocarcinoma of the lung, with N3
metastatic disease as well as ipsi- and contralateral pulmonary metastases.
The diffuse and intense FDG uptake – despite the mucinous nature of the tumor –
is explained by the mucin being intracellular. This differs from mucin lakes
containing only sparse tumor cells, as seen in the cases described above.
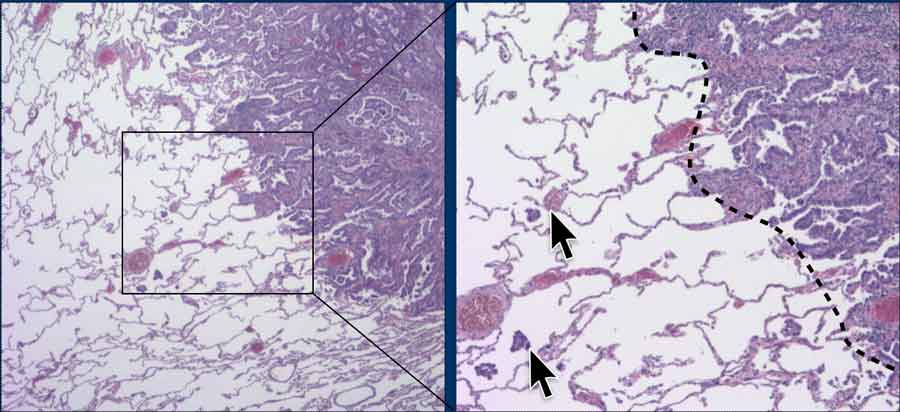
Spread-through-airspaces (STAS)
Images
- Notice tumor noduleswithin alveolar airspaces in the lung parenchyma (arrows) ,
beyond the edge of the main tumor (stippled line).
STAS
Images
- Pneumonic-type lung adenocarcinoma in the left lower lobe, with surrounding nodules due to STAS.
- After lobectomy recurrence occurred with diffuse tumor spread in the contralateral lung, which progressed bilaterally despite systemic treatment.
Progression of Lung Adenocarcinoma
 Subtle progression of adenocarcinoma with lepidic growth
Subtle progression of adenocarcinoma with lepidic growth
The progression of lung adenocarcinoma can differ from that of other primary lung cancer subtypes. When presenting as a solid nodule, progression is readily assessed using diameter measurements or volumetric analysis, similar to other malignancies.
However, adenocarcinomas with subsolid or cystic morphology may exhibit atypical progression due to their distinct growth characteristics and biological behavior.
Ground-glass lesions
These reflect lepidic growth, wherein tumor cells proliferate along intact alveolar walls without invasion or complete airspace filling. This results in the characteristic subtle, infiltrative appearance on CT imaging, which gradually expands over time.
Rather than relying solely on caliper measurements from a single CT slice, progression is better evaluated by assessing the engulfment of adjacent anatomical structures.
Notably, in some cases, an increase in lesion density may accompany a decrease in overall size, despite ongoing tumor progression.
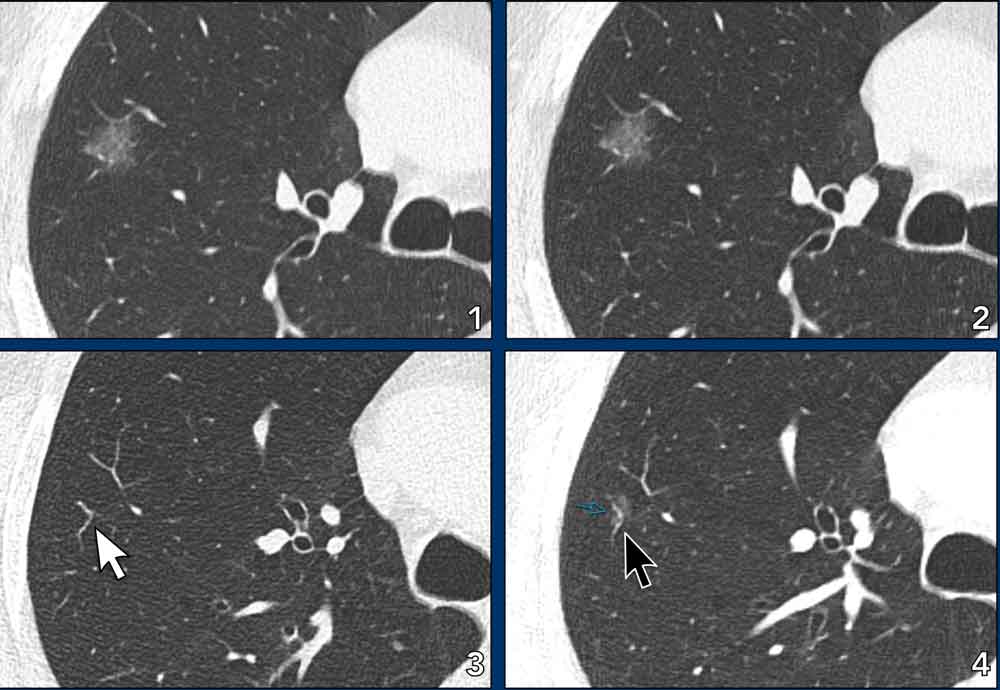
Example
- A simple calliper measurement may show an unchanged diameter, falsely suggesting stability (compare image 1 with 2).
- On closer inspection, however, progression manifests as the ground glass component now surrounds peripheral vessels that were previously unaffected (compare image 3 with 4 (black arrow).
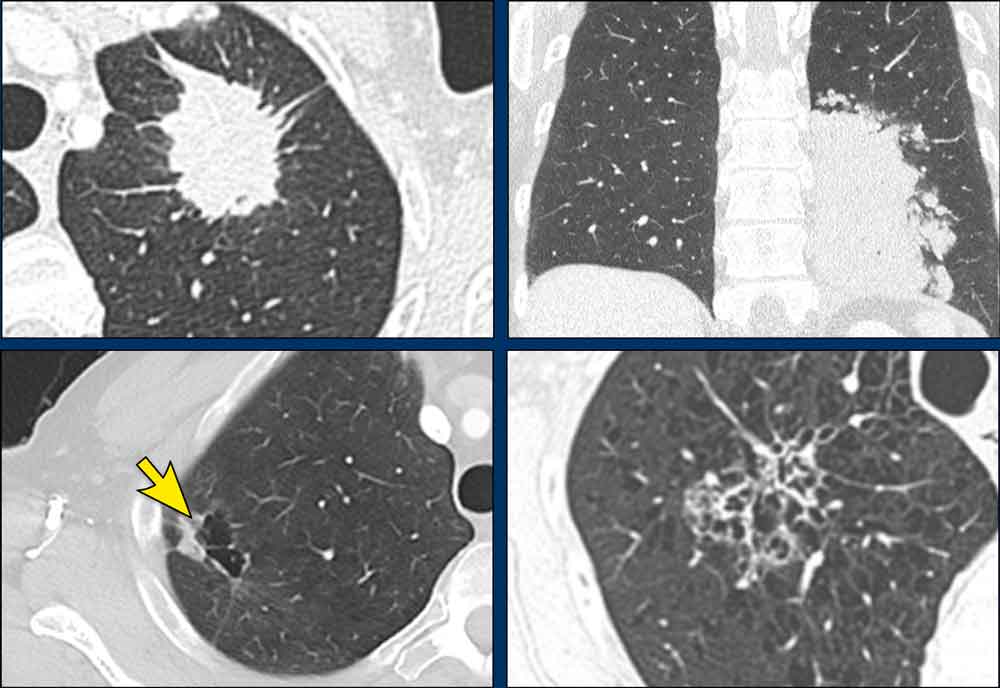
Cystic
adenocarcinomas
These carcinomas may evolve in various ways, including increased lepidic growth,
enlargement of the cystic airspaces, development of focal solid components, and
overall growth. Asymmetric wall thickening or focal tissue growth may represent
the key finding of progression, as tumor cells proliferate along cyst walls.
Notably, lesion morphology can change over time, appearing subsolid, cystic, or
solid depending on the stage at which imaging is performed.
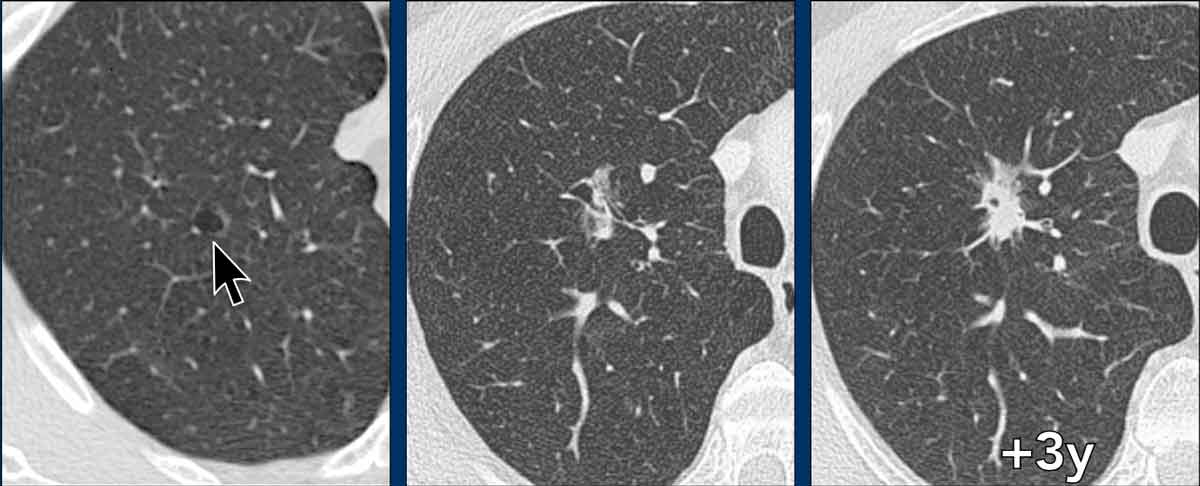
Example
- Adenocarcinoma presenting as a simple cyst , changing into a semi-solid nodule with cystic airspaces, and eventually into a mostly solid lung lesion.
Cystic adenocarcinomas
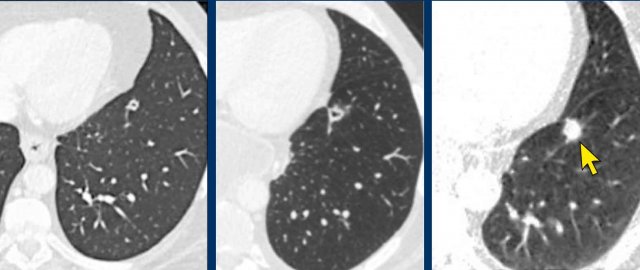
Example
- Adenocarcinoma presenting as a small cystic lesion with irregular wall thickening and progressive overall enlargement, prior to eventual solidification into a small spiculated solid nodule.
Meta- and Synchronous Adenocarcinomas
The exposure to carcinogenic insults — most commonly tobacco smoke — leads to widespread molecular and genetic alterations across the lung.
The entire “field” becomes
biologically primed for malignant transformation (field carcinogenesis), and multiple independent
tumors can develop and may arise at different times and locations.
This helps
explain why synchronous (simultaneous) or metachronous (sequential) primary
lung cancers can be found.
This is relevant in both the initial work-up as well as follow-up in the lung cancer population, where a high index of suspicion is required to enable early detection of other primaries that may influence treatment.
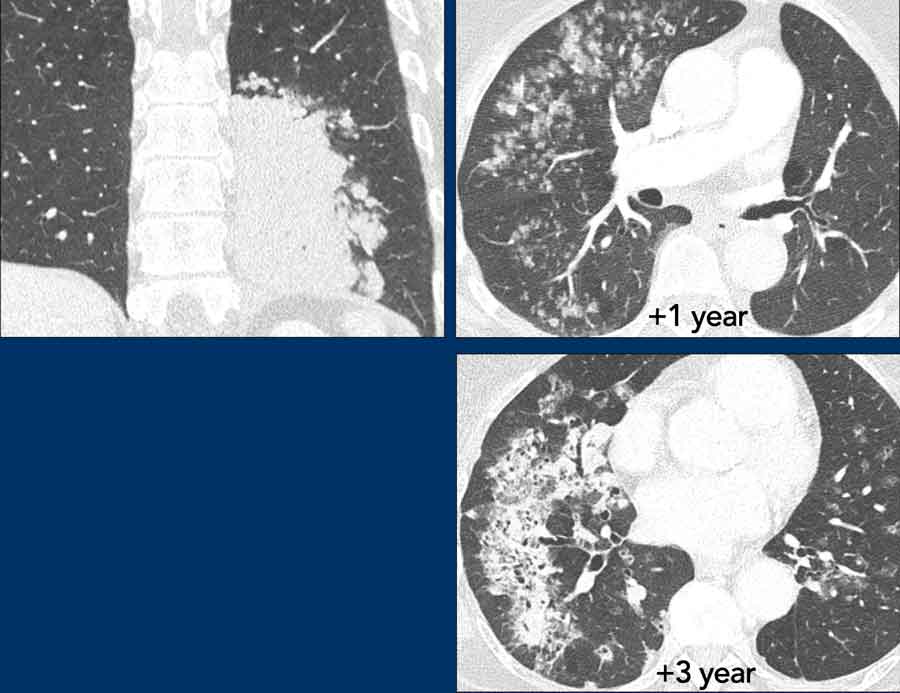
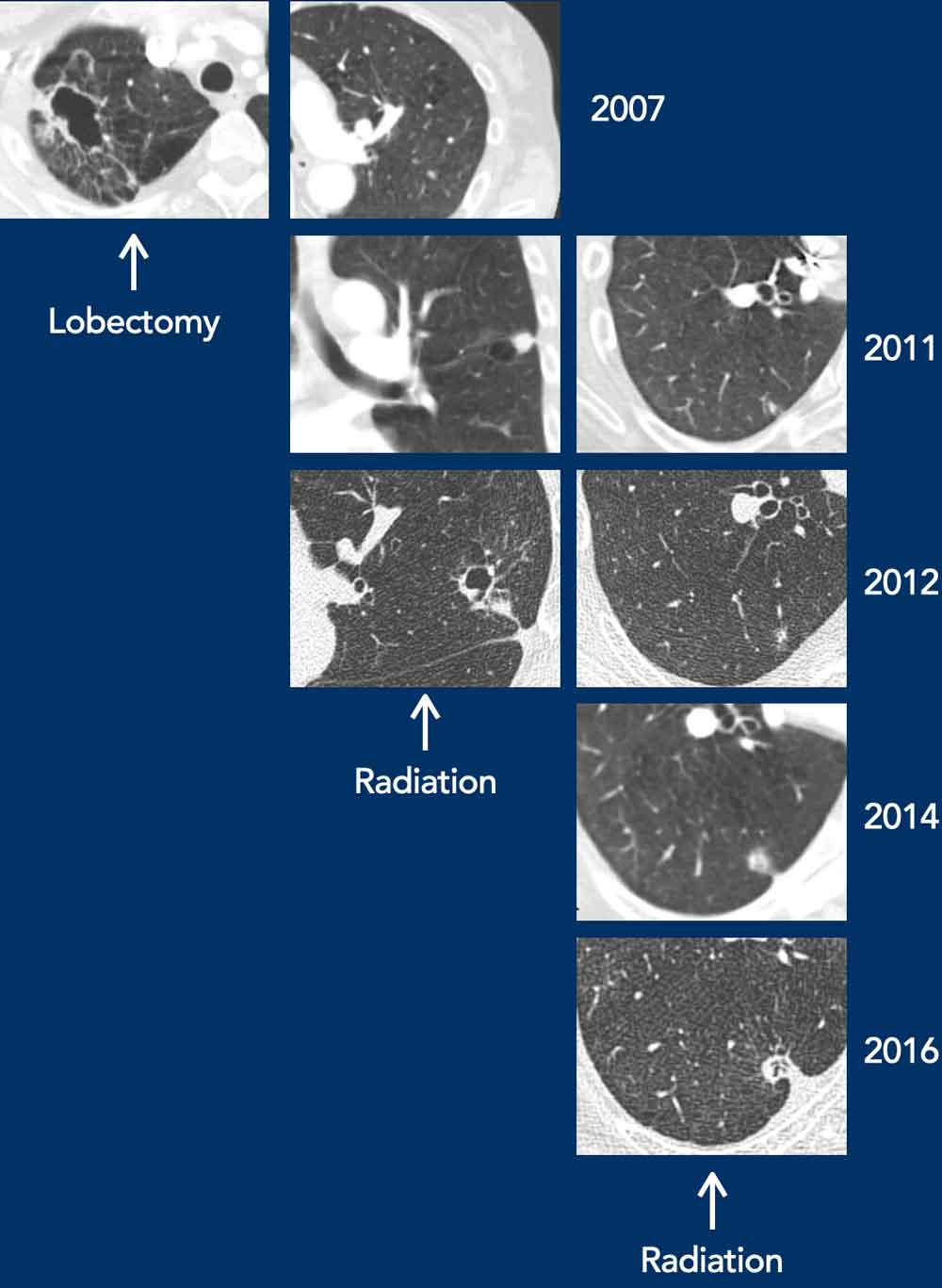
Example of metachronous and synchronous lung cancers
- This patient initially presented with an invasive adenocarcinoma in the right upper lobe, which was treated with lobectomy.
- In the follow-up a cystic lesion developed in the left upper lobe, and was later treated with stereotactic ablative radiotherapy (SABR).
- Meanwhile, in the right lower lobe a subsolid adenocarcinoma progressed, which was later also treated with SABR.

Charity
All profits from The Radiology Assistant are donated to Medical Action Myanmar, an organization led by Dr. Nini Tun and Professor Frank Smithuis Sr.—a professor at the University of Oxford and the brother of Robin Smithuis.
[Watch the Medical Action Myanmar video here.]
If you appreciate The Radiology Assistant, please consider supporting Medical Action Myanmar with a small donation.